Welcome to the Virtual MS Center!
Ask any question you want about Multiple Sclerosis and one of our experts will answer it as soon as possible.
|
Here is My Question:
I am concerned that my wife's WBC has dropped 1/3 in only 6 weeks of using Tecfidera. Initial WBC was 900, and now WBC is 600. I am concerned with a consistent decrease, or is this the normal reduction level? It was suggested to wait 12 weeks for next WBC check up. Is this normal, or should she get it checked sooner? Answer: This is a very good question. First off, I suspect the numbers you provided in your question refer to absolute lymphocyte counts NOT the white blood count or WBC. The WBC includes all the white blood cell types including neutrophils, monocytes, eosinophils and lymphocytes. If these numbers referred to your wife’s WBC, then her counts would have been dramatically low even before starting treatment with tecfidera, since a normal WBC is greater than 3,500. Even absolute lymphocyte counts (ALC) are usually above 900, so if these numbers are correct her counts were low at the beginning of treatment. In my experience lymphocyte counts drop quickly after starting tecfidera with most individuals reaching their lowest counts between 6 and 12 months after start of treatment. The frequency with which blood counts should be monitored in patients on Tecfidera is unclear. I usually do not recheck lymphocyte counts until 6 months after starting the drug. If lymphocyte counts are low, defined as an absolute lymphocyte count less than 600, I repeat the counts in about 1 month. I typically discontinue Tecfidera in anyone with a persistent reduction in absolute lymphocyte counts below 500 for more than one month in the absence of another reason for a low lymphocyte count. Other physicians may discontinue Tecfidera if the low counts persist for more than 3 months. Generally speaking low lymphocyte counts do not immediately increase the risk of infections or tumors; these risks take time to develop unless the counts drop very low very quickly. This is in contrast to low neutrophil counts (as occurs with chemotherapy treatment) which increase the risk of infection immediately. I hope this helps. Revere (Rip) Kinkel, MD Director of the UCSD Multiple Sclerosis Center How long does it typically take for an MS patient to be diagnosed as having MS? Find out in the latest Physician Blog
Q: What are the first symptoms of MS? I know it's different for everyone but what are the most common ones?
A: The first symptoms of MS are too numerous to list and often we are not able to attribute a particular symptom to MS. On the other hand certain syndromes, defined as a collection of symptoms and examination findings occurring in a particular sequence over a designated period of time, are highly characteristic of MS. An example would be a syndrome called optic neuritis where an individual typically experiences pain in one eye when it is moved followed or accompanied by loss of vision in the same eye with maximal deficits usually within a few days, if not sooner. This loss of vision typically involves only the central area of vision, often with preserved peripheral vision. When the visual loss is partial it is typical for the individual to lose color vision in the involved eye. In contrast certain symptoms may be reported by MS patients but are very difficult to directly attribute to MS since these symptoms are often caused by other problems. These non specific symptoms include fatigue, forgetfulness, word finding problems (“tip of the tongue phenomenon”), headaches, and transient pins and needles sensations. Again, while these symptoms are common in MS patients, they are too non specific to be used for diagnostic purposes. Revere (Rip) Kinkel MD Director of the UCSD Multiple Sclerosis Center Q: What is being done about progressive MS? A: Here is a video from MedPage Today that shows what is being done in the area of progressive MS: Stuart D. Cook, MD, of Rutgers-New Jersey Medical School in Newark; Tanuja Chitnis, MD, of Brigham and Women's Hospital in Boston; and Robert Fox, MD, of the Cleveland Clinic's Mellen Center for Multiple Sclerosis are featured in this video. 
Q: When will the mesenchymal stem cell procedure be FDA approved and available in the US?
A: There is no way to know at this time, as there are only preliminary research studies of mesenchymal stem cell transplantation underway in the US. The mesenchymal stem cell transplantation has become very popular in recent years, particularly in Europe. Mesenchymal stem are readily collected from the blood but must be stimulated to proliferate and grow in culture outside of the body to create large enough numbers for transplantation. This procedure does not require risky chemotherapy with ablation of the bone marrow and presumably has a different mechanism of action, if it works at all. There are many private clinics claiming to provide this type of stem cell transplant, but they do not grow and stimulate the cells outside of the body prior to transplantation; it doubtful that this procedure would be of any benefit other than robbing you of hard earned income. There are several preliminary research studies of mesenchymal stem cell transplantation underway with the main US study at the Cleveland Clinic Foundation (Dr Jeff Cohen is the PI). This procedure is still considered experimental and can not be recommended at this time. To learn more about stem cell transplantations, you can read this previously written blog http://www.healthcarejourney.com/q--a-for-virtual-ms-center/stem-cell-transplantation-and-ms Would any of the products advertised for neuropathic diabetic pain help with neuropathy due to MS?
Yes, many of the treatments for pain related to diabetic neuropathy are effective for the painful sensations experienced by MS patients. This includes anticonvulsant class medications such as gabapentin, pregabalin (Lyrica), carbamezipine and topical anesthetic agents such as lidocaine patches. I have had less success with capsaicin cream products and the antidepressant class medications (e.g. amitriptyline, cymbalta) although I still use the latter medications in selected patients. Revere (Rip) Kinkel MD Director of the UCSD Multiple Sclerosis Center Lori Ann Kostich M.S. CCC-SLP
Mandell Center for Multiple Sclerosis Treatment and Research “I want to get back to the way I was.” As a Speech Language Pathologist who works with persons with Multiple Sclerosis (pwMS) I hear this often. PwMS are referred to me by our Neurologist and Neuropsychologist because they report, or demonstrate changes in cognitive –communication or cognitive-linguistic status, and the medical staff believe the pwMS will benefit from a course of therapy. The response I am compelled to give to that initial statement, is, based on the current treatments available, there is no turning back time. The changes in the brain are happening, and they are what they are. The ability to process information slows, and the ability to learn new information (how I think of short term memory) becomes more difficult. But, having said that, therapy from a Speech Language Pathologist, Occupational Therapist, Social Worker, or Psychologist, can be very effective in helping a pwMS manage the changes in cognitive function. Therapists have training and experience helping pwMS develop new routines, change personal habits, make workflow adjustments at the pwMS’ place of employment, and help family members understand the changes the pwMS is experiencing. As part of my practice, I spend a great deal of time doing working on attention and training strategies such as visualization, to help with managing new information. The most important part of each therapy session is asking the pwMS that I am working with how they are going to APPLY what was trained in the therapy session to their daily routines. Therapy addressing cognitive functioning is not like blood pressure medication where you take it and you get better. The onus is really on the pwMS to take the training and strategies home (or to work) and practice them and “tweak” them until whatever issue is better. The most successful outcomes I have had have been when the pwMS worked just as hard outside the therapy setting as they did when sitting across the table from me. Commenting on medications that some of my patient’s claim makes them think better, is out of my scope of practice. So I am not going to. But, please keep in mind that the effects of any medication last only as long as the medication is in a person’s system. In my opinion, it is better to participate in a course of therapy to learn how to manage the cognitive-communication/cognitive-linguistic symptoms for the long term (if you teach a man to fish…). If you are noticing changes in your ability to pay attention, remember new information, or a decrease in your ability to stay organized tell your neurologist, especially if this is affecting your ability to work. A referral can be made to a Neuropsychologist, Speech Language Pathologist, Social Worker etc. Ask for the help. This type of therapy will not make the lesions go away, but it can give you some control over the cognitive changes that are happening. Here is My Question:
What are your thoughts on CBP? Does your center offer cognitive therapy? Do you think medications are more effective than the physical therapy for cognitive function? Answer: Cognitive Behavioral Psychotherapy (CBT) can be helpful in the setting of depression and significant adjustment reaction to the diagnosis of MS. I have used this with good results in some patients. The evidence supports an emphasis on CBT offering coping strategies (which is what some of my patients have found helpful). As with any form of this type of therapy, success is determined--to a degree--on the patient-therapist interaction. On rare occasion, it may be more difficult to find the right personality match between therapist and patient. At our center, we have neuropsychologists who can engage in this type of therapy, and I suspect most comprehensive MS centers have this resource or, at a minimum, a list of good therapists in the community. For cognitive rehabilitation, we use the speech language pathologist in this role but some centers use neuropsychologists, psychologists or social workers for this role. In order to make this effective, we first obtain neuropsychological testing (in the appropriate individual) which is a battery of tests that determine an individual's strengths and weaknesses in respect to their cognitive function. Once the pattern of deficits is understood, a tailored rehab program can be created and implemented. This is also a helpful modality of treatment. MS research has evaluated various medications that are used in other cognitive diseases (such as Alzheimer's and other cognitive impairment/memory diseases). Unfortunately, the results have been mixed at best, but typically disappointing. When I think of medicine and cognitive problems in MS, I first think about medication I can remove from a patient's medicine cabinet. Many of the symptomatic medications we use in MS can have the side effect of cognitive dysfunction. For more information on cognition and MS, please see Dr. Kinkel's blog. Hope this helps, A. Scott Nielsen MD, MMSc Virginia Mason Multiple Sclerosis Center Seattle, WA In the latest newsletter from the Rocky Mountain MS Center, we found this article on the Medicaid Buy-In which we thought was interesting so we wanted to let you know about it. If the font below is too small, the link to the newsletter is here and the article is on page 18. 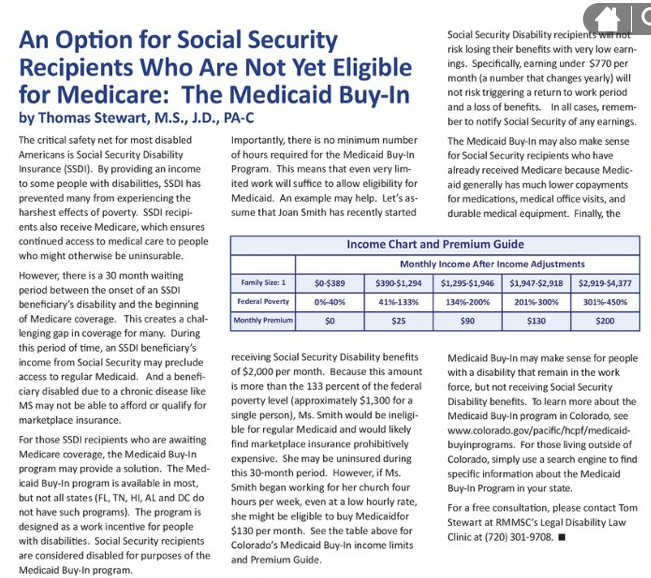 Here is My Question:
I have just been diagnosed with RRMS. The most troublesome symptom that I struggle with is the cognitive deficits. I used to be a full functioning store manager and bread winner of my family. I am now on the verge of losing my job with no income. Is there medication or treatment to reverse or fix the forgetting, concentration, unable to make decisions? My doctor ordered Tecfidera...will that help? There are no MS specialists in Yuma. Answer: We are sorry to hear that your MS is impacting your job. There are many resources for you to turn to, so we will do our best to inform you of them in this blog so that you are able to get the best care and treatment and resources for you and your family. Here are a few blogs on cognitive dysfunction and MS that might be helpful for you to read in terms of what happens cognitively and what you can do to help manage it: BLOG 1 BLOG 2 There are two great articles in this newsletter from the Rocky Mountain MS Center that address both disability insurance/job benefits as well as cognition that you definitely will want to read: http://catalog.proemags.com/publication/b860b13c#/b860b13c/1 The Rocky Mountain MS Center also has a free consultation for people with MS nationally regarding employment/job benefits (you can call for a free consultation at (720)301-9708) The National MS Society has a chapter in Arizona (you can call them at 1-800-344-4867) that you might contact as they may have recommendations for you in terms of neurologists in your area with MS experience as well as resources regarding job related issues: National MS Arizona Chapter. There might not be any MS specialists in Yuma (you can check with the NMSS), but Dr. Revere Kinkel who blogs on this site and is a MS specialist is at the University of California San Diego MS Clinic which is only 2.5 hours from Yuma, so you can consider that as an option as well. The number for his clinic is (858) 822-5861 and here is a link to their website UCSD MS CLINIC. Question:
If the Epstein-Barr virus is thought to be connected to MS, is it possible that I got that virus from a woman I worked with for four years, which then led to my MS? My co-worker was diagnosed with PPMS during our first year of working together, and her husband's first wife was diagnosed with MS several years before that. This seems like too much of a coincidence. Thanks. Answer: The association between viral infections and MS have been studied for decades. Most of the studies have failed to reveal a direct cause and effect relationship. The best data suggests that if the “right” person gets exposed to Epstein-Barr virus at specific times in their life, then their risk of MS goes up significantly. So, it is not as simple as a coworker passing along a virus. The Epstein Barr virus is ubiquitous – it could come from anyone and usually someone with close contact to a person, not a casual co-worker. Beyond this, it is worth noting that MS is actually a common disease. With a prevalence of 1 in 900, it is rare for a person in the US NOT to have contact with people with MS. Thus, while there definitely could be a link to meeting people with MS, the disease was probably triggered years before that meeting occurred. Benjamin M. Greenberg, MD, MHS Director, Transverse Myelitis, Neuromyelitis Optica and Pediatric Demyelinating Disease Programs Director, Neurosciences Clinical Research Center UT Southwestern Medical Center Childrens Medical Center Dallas, Texas Here is My Question:
I am a 66 year old male recently diagnosed with MS with 1 documented relapse. Given my age, a history of Celiac disease, hypothyroidism, and recent pulmonary embolisms 2 months before 1st presentation of optic neuritis, what would be the appropriate MS med to prevent relapses & progression of MS? I need to continue taking Coumadin & Synthroid as well as Lisinopril. Thank you! Answer: Call me a skeptic, but I get concerned when I hear about a 66 year old man newly diagnosed with MS, especially when it appears to be of a relapsing type. I certainly do see individuals in this age group with a new diagnosis of MS, but this diagnosis requires additional assurance and diagnostic evaluations for various reasons in your age group. For instance you have a diagnosis of Celiac disease which is associated with the development of non specific white matter lesions on MRI in the absence of MS. You have also recently experienced pulmonary embolisms which are very usual in individuals who are not ill or immobile, unless you have an underlying condition predisposing you to blood clot formation. Some of these underlying conditions, such as anticardiolipin antibody syndrome, are associated with neurological symptoms. Lastly, you were told you experienced optic neuritis. Depending on your symptoms, exam findings and degree of recovery I would be more concerned about a diagnosis of Anterior ischemic optic neuropathy (AION) or a neuromyelitis optics spectrum disorder in a gentleman of your age. Please make sure your neurologist has considered these issues and obtained spinal fluid for examination that showed findings consistent with MS before proceeding further with treatment Good luck Rip Kinkel MD Director, University of California San Diego MS Center  I will answer this question under the assumption that the "journey" asked about is regarding a disease modifying therapy (DMT) called interferon-beta 1a (also known as Avonex). This DMT is injected into the muscle once weekly and was approved by the FDA for the treatment of relapsing multiple sclerosis.
Once injected (about 1 milliliter) into the muscle, absorption of the drug occurs and reaches the blood circulation which delivers it throughout the body. The active ingredient is a Type I interferon (which is identical to interferon made in our bodies as a response to a viral infection). The interferon is simply a string of protein building blocks (or amino acids) that also has a sugar chain attached to it. This complex (protein and sugar) interacts with receptors on various cells in our body (think of a lock and key relationship where the interferon is the key and the receptors are the locks). When the interferon unlocks the receptor on the surface of different cell types, it causes various chemical reactions inside the cell. One of these reactions includes the movement of a protein complex into the nucleus of our cells (this is the part of the cell that houses our DNA--or genetic code). This protein complex attaches itself to part of the machinery of the cell nucleus that expresses our DNA. (This machinery is like a Xerox copy machine of sorts. It recognizes specific genes and can literally copy the genes or translate the genetic code into other proteins that can leave the nucleus and do work that needs to be done throughout our body.) In the case of interferon, the machinery induces the expression of genes to fight viruses, provide anti-proliferative signals, and "modulate" the immune system. It is the induction of these "modulatory" genes that presumably exert the beneficial effects in MS patients (ultimately reducing the bad inflammation in the brain and spinal cord, the number of MS attacks, new scars on the MRI scans, and reduce the accumulation of physical disability over time). Clinical trial evidence suggests that the intramuscular (IM) route of administration was superior to intravenous (IV) but comparable to subcutaneous (just under the skin) in the sense that IM and subcutaneous injection reached a peak of biological effect at 48 hours rather than 24 hours by the IV route). Also the overall exposure (what we term the "area under the curve" when we plot blood levels of biological response markers over time after the injection) to the interferon was greatest using the IM route compared to IV or subcutaneous injections. Interferon is metabolized (ie, digested) by the liver as many drugs are, and eliminated from the body primarily through our kidneys. The half-life (the time it takes to half the amount of drug in the blood stream) is approximately 19 hours. A. Scott Nielsen MD MMSC Virgina Mason Multiple Sclerosis Center Here is My Question:
I am a 54 year old female diagnosed with transverse myelitis and MS in 2001. I also have gastroparesis, PFD and IBS. My question concerns a vago response (like benign cough headache) that occurs when I have an IBS attack. Bowel movement starts out normally, but continues until I start feeling nausea. When I wretch or start to vomit, I get an instant violent headache that literally puts me on the floor for a couple of minutes. The headache is so severe and violent that my neurologist gave me an MRI and MRA which showed nothing. I have been having these for years and the only way to prevent them is to not have an IBS attack. What are your thoughts on this? Could it be from jugular vein? Should I see cardiologist? I'd really like to know what is happening. They are very scary. Answer: These sudden headaches could certainly be caused by the primary or secondary cough headache syndrome. Cough headaches do not need to accompany a cough; simply straining, vomiting or any other activity that suddenly increases intrathoracic pressure can trigger these headaches. Primary cough headaches are generally intermittent, rare and brief without any known cause. Secondary cough headaches are caused by conditions that lead to a sudden rise in the pressure in your head; many of these conditions can be detected by an MRI scan. Rip Kinkel MD Director, University of California San Diego MS Center PLEASE NOTE: The information/opinions on this site should be used as an information resource only. This information does not create any patient-HCP relationship, and should not be used as a substitute for professional diagnosis and treatment. Please consult your health care provider before making any healthcare decisions or for guidance about a specific medical condition. As HealthCare Journey learns about what MS Clinics around the country are doing for patients like the Rocky Mountain MS Center in Denver, we would like to offer you some of the great educational materials they are creating. Our goal is to share this knowledge with everyone regardless of whether the clinic is in your area so we can all learn and benefit from their expertise. The Rocky Mountain Center has been gracious enough to share their educational materials with us. Here is the first (see link below) A big "THANK YOU" to them!
InforMS- Fall 2014 Question:
I take Ampyra and I am on social security disability thru United Health Care. They spent 50 cents to write and tell me that Ampyra would not be covered by them in 2015...I also have read that there is a generic Ampyra in the works. Is the info about Ampyra true? Answer We contacted Acorda (the maker of Ampyra) and they suggested you contact their support services group at 1-888-881-1918. They will be able to provide assistance specific to your situation. Here is My Question:
I have a person telling me that my silver fillings are what is causing my MS. They want me to go and have them all removed. It doesn't make sense to me, but I was hoping any of you might have some insight into this. Thank You Answer: There is no data to suggest silver filling is associated with, let alone causes, multiple sclerosis. I would not suggest removing them unless there is an orthodontic reason to do so. A. Scott Nielsen MD, MMSc Virginia Mason Multiple Sclerosis Center Question: Is there an organization that can help financially for a MS patient to get a wheelchair lift and ramp? One local company wants over $3,000 and I can't afford that. Please help. Answers: 1) In seeking financial assistance for non-covered items, a lot will depend on where you live. Many MS Regional Chapters can offer assistance through their location and/ or National MS headquarters. They will require you to fill out some financial forms to show the need. You can also find private groups like Moose Lodges, ‘Nice Guys’ (this is in the San Diego area), or church groups, all of which are good secondary sources for funding. I hope that this is somewhat helpful. -Tom Mellor- Assistive Technology Professional at the Mobility Center (telephone 8585420552) 2) I have attached literature that I received from an MS conference on financial assistance for vehicle and home modifications (this contact information on the form is for the Northeast chapter). Also, another source for financial assistance is the Rockville Roadies MS Project and their website is http://rockvilleroadies.com/. I hope this helps and please e-mail or call me anytime. -Eric Lajeunesse- Mobility Consultant at Ride-Away Handicap Equipment Corporation (telephone 6032163910; email [email protected])
|
PLEASE NOTE: This information/opinions on this site should be used as an information source only. This information does not create any patient-HCP relationship, and should not be used as a substitute for professional diagnosis and treatment. Please consult your health care provider before making any healthcare decisions or for guidance about a specific medical condition.
Archives
June 2024
Categories
All
|
||||
|
|
© 2023 HealthCare Journey, LLC. All Rights Reserved. HealthCare Journey™ is a trademark of HealthCare Journey, LLC |
|
 RSS Feed
RSS Feed