Welcome to the Virtual MS Center!
Ask any question you want about Multiple Sclerosis and one of our experts will answer it as soon as possible.
|
Here is My Question:
I work outside 4 hours a day. I am required to wear a mask at all times. When I am done I have a bad headache and I feel weak (my legs are like noodles). Does wearing the mask effect my MS? Answer: Wearing a mask should have no effect on your MS. Check the air quality in your area using the AirNow app from the EPA (download from the app store). Poor air quality from high ozone or particles could be contributing. You should also contact your primary care physician about these symptoms Good luck Revere P (Rip) Kinkel, MDProfessor of Clinical Neurosciences Director of the Multiple Sclerosis Program Clinical Neurosciences Director University of California San Diego
0 Comments
Here is My Question:
My daughter's MRI says the T2 and flair hyper intense lesions are 15-20 in the supratentorial white matter suspicious for demyelination. Does this mean it is likely MS? She is only 15. Answer: There are many causes of T2/FLAIR hyperintense lesions in the supratentorial white matter of people at any age. The differential diagnosis depends on the medical history and symptoms, exam findings, family medical history and, to a great extent, on the age of the individual. The presence of T2/FLAIR hyperintense lesions is by no means diagnostic of MS by itself. Revere P (Rip) Kinkel, MDProfessor of Clinical Neurosciences Director of the Multiple Sclerosis Program Clinical Neurosciences Director University of California San Diego Here is My Question:
Hi, I will start a laser hair removal next week. I have been taking Gilenya for 8 years. Is there any danger? Thank you! Answer: I know of no contraindication to laser hair removal related to the use of Gilenya Good luck Revere P (Rip) Kinkel, MDProfessor of Clinical Neurosciences Director of the Multiple Sclerosis Program Clinical Neurosciences Director University of California San Diego Here is My Question:
Would Kesimpta be a good alternative to Ocrevus if I'm worried about potentially being exposed to COVID during an infusion? Do you know if I might experience a rebound after discontinuing Ocrevus? Is there an optimal amount of time after stopping Ocrevus before starting Kesimpta? And lastly, does the fact that Kesimpta has to be administered every month vs every 6 months mean my immune response might come back more quickly if I get COVID and stop taking it while I fight the disease? Many thanks! Answer: Very good questions about switching from Ocrevus to ofatumumab (Kemsimta). Here are my responses
Director of the Multiple Sclerosis Program Clinical Neurosciences Director University of California San Diego Here is My Question:
How come I get cuts after my bruises goes away? Answer: Questions regarding cuts and bruises should be directed to your primary care physician since there are many potential explanations most of which have no relationship to your multiple sclerosis. Revere P (Rip) Kinkel, MDProfessor of Clinical Neurosciences Director of the Multiple Sclerosis Program Clinical Neurosciences Director University of California San Diego Here is My Question: Does the number of oligoclonal bands found in CSF determine the prognosis of your MS? What is an”median” number of bands found in someone with MS? My LP revealed 14 bands and I wondered how this relates to my MS diagnosis and prognosis? Answer: The term "CSF (Cerebrospinal Fluid) Oligoclonal bands", or sometimes shortened to Oligoclonal bands, refers to the presence of several unique immunoglobulins (also called antibodies) in the spinal fluid that cannot be identified in a matched plasma sample. This is a qualitative test that requires some experience for the identification of the individual band number in the sample. The proteins within the body fluid being sampled (plasma or CSF or whatever) are separated on an agarose gel by their size and electrophoretic properties (remember, proteins have an electric charge) and stained for visualization. The staining process reveals the migratory location of the various proteins on the gel for visualization (see below). Counting individual bands can be difficult if they are faint or overlap with other protein bands, but various techniques have been developed over the years to improve the resolution of the assay. The picture that follows (reproduced many times in other publications and online) gives you an idea of the qualitative nature of the assay. The left-hand panel for both the normal and abnormal patient (abnormal referring to the one with multiple sclerosis) is the CSF banding pattern and the right-hand panel on each side is the plasma sample from the same person. It is easy to identify the different staining patterns in the CSF immunoglobulin region from the person with MS compared to the "normal" person without MS (both labeled), but I challenge you to count the number of bands in this region from the CSF sample that are not present in the adjacent plasma sample. 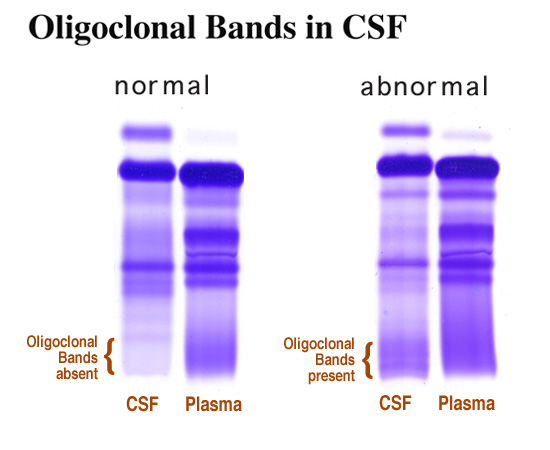 So, this is how the assay is done. What does it mean? The presence of 2 or more CSF oligoclonal bands is a sensitive diagnostic marker for MS in the correct clinical circumstances(positive predictive values of 95 % in some circumstances).This means that CSF oligoclonal bands can be seen in other conditions and cannot be used alone to diagnose MS but is extremely useful and predictive in the right circumstances.
More recent studies suggest that the number of oligoclonal bands is predictor of disease severity. In one study of people with a first attack of MS, the median number of oligoclonal bands at onset was 8 and those individuals with more than 8 oligoclonal bands at onset experienced more disease activity. In another study of people with known MS on DMTs, those with greater than 10 oligoclonal bands experienced a worse prognosis. At present there is no accepted cut off for a number of oligoclonal bands that indicate a worse prognosis. We prefer to use several pieces of information, including the number of CSF oligoclonal bands, to make this assessment. This information may include other biomarkers such as CSF free kappa light chains or serum neurofilament light chain measurements. These are particularly good measures because of their associations with disease activity and severity and the quantitative and sensitive nature of the assays used. We also use demographic features (age and sex), clinical features, responses to prior treatments and MRI measurements to help with prognostication. Hopefully, we will be able to develop a panel of measures in the future that when combined allow us to both prognostic risk of disease activity and response to treatment. Revere P (Rip) Kinkel, MDProfessor of Clinical Neurosciences Director of the Multiple Sclerosis Program Clinical Neurosciences Director University of California San Diego |
PLEASE NOTE: This information/opinions on this site should be used as an information source only. This information does not create any patient-HCP relationship, and should not be used as a substitute for professional diagnosis and treatment. Please consult your health care provider before making any healthcare decisions or for guidance about a specific medical condition.
Archives
June 2024
Categories
All
|
|
|
© 2023 HealthCare Journey, LLC. All Rights Reserved. HealthCare Journey™ is a trademark of HealthCare Journey, LLC |
|
 RSS Feed
RSS Feed