People with MS often experience loss of strength in certain muscle groups. The irony is that there is absolutely nothing wrong with the muscles themselves and usually nothing wrong with the peripheral nerves that innervate (electrically stimulate) the muscles to make them contract.
So why does leg weakness occur if nothing is wrong with your legs? The problem results from interrupted or dysregulated electrical signals passing down the spinal cord to the motor neurons in the spinal cord, or from damage to the motor neurons or axons within the spinal cord. This creates certain patterns of weakness early in the disease that should be easily recognized by a neurologist.
The muscle groups affected first tend to include the:
So why does leg weakness occur if nothing is wrong with your legs? The problem results from interrupted or dysregulated electrical signals passing down the spinal cord to the motor neurons in the spinal cord, or from damage to the motor neurons or axons within the spinal cord. This creates certain patterns of weakness early in the disease that should be easily recognized by a neurologist.
The muscle groups affected first tend to include the:
- hip flexors (the muscles that lift your leg off the ground at the hip joint while seated or lying down)
- hip adductors (the muscles that slide your legs together if you are lying down or sitting with them apart)
- ankle dorsiflexors (these are the muscles that bring the foot up if you wiggle your foot up and down at the ankle joint)
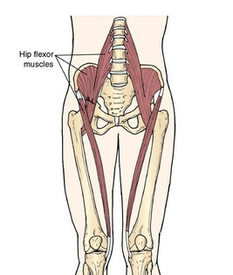
Source: http://www.newhealthguide.org/Hip-Flexor-Strain.html
|
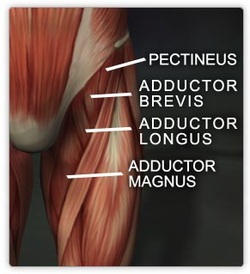
Source: http://www.realbodywork.com/learn/hip/adductors.jpg
|

Source: http://taylorednutrition.tripod.com/heelup.html
|
Eventually, as the disease progresses all muscle groups can be affected. This pattern of weakness is usually accompanied by an increase in reflexes when the doctor taps on you with a reflex hammer and an increase in muscle tone when the legs are rapidly moved by the doctor which we call spasticity. To learn about spasticity, go to http://www.healthcarejourney.com/spasticityspasmscramps.html
Gait Abnormalities
This entire pattern is called upper motor neuron weakness and creates common gait difficulties (abnormalities in the way you walk). When you walk you may appear slightly stiff (or very stiff depending on the severity) and this problem will be more noticeable the faster you walk. If you are able to jog it will become very noticeable. If the muscles around the hip are particularly affected, there is a significant lag noticed with bringing the affected leg forward in walking. This will often result in:
If the ankle dorsiflexors are weak, your walking may have a steppage quality (the leg is lifted higher when swung forward so that the toes clear the ground) or you may just drag the toes or inside of the foot on the ground as the leg moves forward. If both legs are affected, this pattern will alternate back and forth as you walk often creating a seesaw appearance remotely similar to the way Charlie Chaplin would walk in his old silent movies. We call weakness of this type in both legs a spastic paraparesis; weakness of this type in only one leg is called spastic monoparesis. Weakness can often be compensated for with the use of appropriate exercises and assistive devices, including braces, canes or walkers.
Spastic Weakness and Compensatory Gait
Spastic weakness in one or both legs is a common symptom of MS. When this occurs, people sometimes compensate by walking differently. This is known as a compensatory gait. Walking with a limp, swinging one leg in a circle or hiking up a hip to prevent tripping are all examples of a compensatory gait.
People with compensatory gait sometimes complain of back, hip or knee pain. They may also develop heel pain from a excessive heel strike while walking. Their discomfort may likely be due to the change in their walking pattern, and thus is a secondary symptom or complication of weakness in their legs. In addition, when weakness occurs, a person may have reduced stamina when standing or walking. The usual result is less activity, which can cause another secondary symptom known as disuse weakness. Muscles become deconditioned and weaken further.
Weakness and compensatory gait patterns must be identified early so that appropriate steps can be taken to prevent the secondary symptoms or complications of pain and disuse weakness. An early referral for physical therapy is the best way to improve walking and avoid these problems.
The above content was written by Revere Kinkel, MD, published March 28, 2014
© Copyright 2014 Healthcare Journey, LLC All rights reserved.
Gait Abnormalities
This entire pattern is called upper motor neuron weakness and creates common gait difficulties (abnormalities in the way you walk). When you walk you may appear slightly stiff (or very stiff depending on the severity) and this problem will be more noticeable the faster you walk. If you are able to jog it will become very noticeable. If the muscles around the hip are particularly affected, there is a significant lag noticed with bringing the affected leg forward in walking. This will often result in:
- “vaulting” (a compensatory technique that involves raising the heel on the stronger leg to make it easier to swing the weaker leg forward)
- compensatory hip hike (your upper body rises up on the affected side to lift the leg forward)
- circumduction (swinging the leg outward as it moves forward). Your trunk may also lean away from the weak leg.
If the ankle dorsiflexors are weak, your walking may have a steppage quality (the leg is lifted higher when swung forward so that the toes clear the ground) or you may just drag the toes or inside of the foot on the ground as the leg moves forward. If both legs are affected, this pattern will alternate back and forth as you walk often creating a seesaw appearance remotely similar to the way Charlie Chaplin would walk in his old silent movies. We call weakness of this type in both legs a spastic paraparesis; weakness of this type in only one leg is called spastic monoparesis. Weakness can often be compensated for with the use of appropriate exercises and assistive devices, including braces, canes or walkers.
Spastic Weakness and Compensatory Gait
Spastic weakness in one or both legs is a common symptom of MS. When this occurs, people sometimes compensate by walking differently. This is known as a compensatory gait. Walking with a limp, swinging one leg in a circle or hiking up a hip to prevent tripping are all examples of a compensatory gait.
People with compensatory gait sometimes complain of back, hip or knee pain. They may also develop heel pain from a excessive heel strike while walking. Their discomfort may likely be due to the change in their walking pattern, and thus is a secondary symptom or complication of weakness in their legs. In addition, when weakness occurs, a person may have reduced stamina when standing or walking. The usual result is less activity, which can cause another secondary symptom known as disuse weakness. Muscles become deconditioned and weaken further.
Weakness and compensatory gait patterns must be identified early so that appropriate steps can be taken to prevent the secondary symptoms or complications of pain and disuse weakness. An early referral for physical therapy is the best way to improve walking and avoid these problems.
The above content was written by Revere Kinkel, MD, published March 28, 2014
© Copyright 2014 Healthcare Journey, LLC All rights reserved.
Managing Leg Weakness
Now that you've reviewed a lot of information here about leg weakness, we would like to offer some suggestions about taking control of some of these symptoms. Yes, you can do something about your leg weakness! It's so important to develop an exercise program early on (or later). Physical therapists can be an invaluable resource for you, but you need to go to a therapist who is familiar with MS.
There are two important points to consider in finding the right care for your MS needs:
- Finding the right physical therapist (PT) - PTs can specialize just like doctors. A PT who specializes in treating neurological and balance deficits often offers the best care for MS.
- Finding the right setting - Look for outpatient neurologic therapy if it is available in your area. MS specialists are more often in the outpatient neuro departments, but can sometimes be found in home health.
A great place to start looking for a physical therapist in your area is through the American Physical Therapy Association (APTA) specialists website. Check out their website for someone with a Neurologic Certified Specialist designation (NCS). http://www.apta.org/apta/findapt/index.aspx?navID=10737422525. Your local MS organizations (NMSS or MSAA) can also help assist you in finding an experienced therapist. You will need a prescription from your health care provider for physical therapy so you need to be your own advocate and ask to see a therapist. Early intervention is the best way to help prevent complications.
Wearing the right shoes is very important. Click here to read more. http://www.momentummagazineonline.com/shoe-fits/
|
|
|
Here is a great resource from the National MS Society on choosing the best mobility device for you (click on the "Download File" in blue below)
| mobilityguide.pdf |
Products and Services for Leg Weakness
Question from a person with MS:
"Is there anyone who has found a scooter that is less than 40 lbs? All of the ones I have seen are at least 70-80 lbs. I am not able to get around without a scooter and would like to be able to shop without my husband."
Recommendation:
TravelScoot
The Travelscoot standard model (see website below) weighs 30 lbs without battery. Remove the seat and seat back, and it weighs less than 24 lbs.
There is also a shopper model that weighs just over 26 lbs. Without the seat and battery it weighs just 15 lbs. With a top speed of about 2.3 mph, it is suitable for crowded environments such as shopping centers, pedestrian zones, fairs, museums and exhibitions. The maximum load is 320 lbs.
http://www.travelscoot.com
Question from a person with MS:
"Is there anyone who has found a scooter that is less than 40 lbs? All of the ones I have seen are at least 70-80 lbs. I am not able to get around without a scooter and would like to be able to shop without my husband."
Recommendation:
TravelScoot
The Travelscoot standard model (see website below) weighs 30 lbs without battery. Remove the seat and seat back, and it weighs less than 24 lbs.
There is also a shopper model that weighs just over 26 lbs. Without the seat and battery it weighs just 15 lbs. With a top speed of about 2.3 mph, it is suitable for crowded environments such as shopping centers, pedestrian zones, fairs, museums and exhibitions. The maximum load is 320 lbs.
http://www.travelscoot.com
Other Products and Services
- Learn about recommended scooters for people with MS
- A blog about a product to help you keep walking if one or both legs are weak
- Our patient blog with some tips for going to a show or concert
- Great app designed by someone with MS to help those in wheelchairs
PLEASE NOTE: The medical information on this site is provided as an information resource only, and is not to be used or relied on for any diagnostic or treatment purposes. This information does not create any patient-physician relationship, and should not be used as a substitute for professional diagnosis and treatment. Please consult your health care provider before making any healthcare decisions or for guidance about a specific medical condition.