Welcome to the Virtual MS Center!
Ask any question you want about Multiple Sclerosis and one of our experts will answer it as soon as possible.
|
Here is My Question:
What can you tell me about Tecfidera depressing white blood cell counts? I am trying to decide between it and Copaxone and want to be informed. Answer: Your white blood count or WBC includes many different cell types including neutrophils, monocytes, eosinophils and lymphocytes. All have different functions and loss of individual cell types can have different consequences. For instance, chemotherapies used to treat cancer can suppress neutrophil counts and make patients susceptible to bacterial and fungal infections. Suppressed lymphocyte counts have less predictable effects but when severe and prolonged, such as occurs in patients with HIV infection, can lead to unusual infections only seen in patients with suppression of normal immunity. Tecfidera decreased mean lymphocyte counts by 30% in the phase III clinical trial that led to its approval by the FDA. This means the investigators compared the average of all the lymphocyte counts in all the patients on Tecfidera in the trial at each time point and compared this average number to those on placebo and the counts were 30% lower in the Tecfidera group. This does not mean that 30% of patients on Tecfidera experience a drop in lymphocyte counts. Overall this is considered a relatively mild and insignificant drop in lymphocyte counts. In fact the mean lymphocyte counts in patients on Tecfidera remained well above the lower limit of normal (lower limit of normal is a below a count of 900). Only 6% of patients experienced a drop in lymphocyte counts below 500 in the trial compared to 1% of patients on Placebo. This is reason that we need to monitor your lymphocyte count while taking Tecfidera; if your count remains below 500 on repeated testing over time and there is no other explanation (such as another medication or illness), then your physician may consider stopping the Tecfidera. There was no evidence that patients on Tecfidera were more susceptible to infections as a result of this drop in lymphocyte counts during the study which lasted for 2 years, but there remains a concern that a prolonged drop in lymphocyte counts could lead to an increased risk of infections over years of treatment. Other MS drugs that cause drops in lymphocyte counts include the interferons (Avonex, betaseron, Extavia and Rebif), Gilenya and Aubagio. The drops in lymphocyte counts are most dramatic with Gilenya (73% reduction in mean lymphocyte counts compared to placebo) but Gilenya has only been associated with a mild increased risk of respiratory tract infections and herpetic infections (e.g.. shingles) and this infection risk has not been necessarily linked to the reduction in lymphocyte count. Rip Kinkel, MD Here is My Question:
I have narrowed it down to Tecfidera and Copaxone and would appreciate a clinical and real life comparison of the two. My concern with Tecfidera is long term effects, since the long term effects of Copaxone are apparent due to its longevity on the market. So Copaxone or Tecfidera and why? Answer: This is a really good question but I doubt my answer will be of value to you. I can provide comparisons of the two drugs but advising an individual patient on a particular drug requires knowledge of that individual’s disease characteristics. So what are the comparisons between Copaxone and Tecfidera? It just so happens that one of the clinical trials of Tecfidera used Copaxone as an unblinded comparison arm so we have some information available to compare these two therapies. The clinical trials results over two years for each of drugs compared to a group receiving placebo was as follows:
Rip Kinkel Question:
Is PLEGRIDY another interferon? How might it be different from the interferons already used in the treatment of MS? Answer: PLEGRIDY is pegylated interferon 1-a, the same active interferon molecule used in the branded drugs, Rebif and Avonex. Pegylation is the process of covalently attaching polyethylene glycol polymer chains to a protein, to increase its duration of action by slowly releasing the active molecule. This has been done with several other biological molecules used to treat other diseases like rheumatoid arthritis. Because of the pegylation process, PLEGRIDY only needs to be administered every 2 weeks by subcutaneous administration but with the usual interferon side effects. The clinical trial results with PLEGRIDY were nothing short of amazing for a first line therapy; the Advance study (PLEGRIDY clinical trial in relapsing MS) reported a 36 % reduction in relapse rate and a 38 % reduction in sustained disability progression over 1 year compared to placebo. There were also significant reductions in MRI activity and a very low rate of neutralizing antibody formation. The FDA is still reviewing the drug application for PLEGRIDY but I suspect it may replace most interferons as first line therapy if it is as well tolerated as reported and the costs are reasonable compared to other first line agents for MS. Rip Kinkel, MD PLEASE NOTE: The information/opinions on this site should be used as an information resource only. This information does not create any patient-HCP relationship, and should not be used as a substitute for professional diagnosis and treatment. Please consult your health care provider before making any healthcare decisions or for guidance about a specific medical condition. Here is My Question: My daughter has been on Tysabri for almost 4 1/2 years. At the end of year 2 she was put on "holiday" and after 3 months had what seemed to be a relapse but was in fact declared IRIS. She received steroids and was immediately put back on Tysabri. At the time, she was told that she could never come off Tysabri. Fast forward 2 1/2 years. Her JC virus antibody values have tripled in the past nine months and are now at 1.3. This would suggest coming off Tysabri but what about the IRIS? Answer: The risk of PML on Tysabri is related to duration of therapy over two years, JCV antibody index and whether or not a patient has received prior immunosupression. For my response I will assume your daughter has not been treated with an immunosuppressant in the past. According to our current understanding of these risk factors (CLICK HERE to read my previous blog on Tysabri risk), your daughter’s current risk of PML is approximately 1 in 1,000 or 0.1%. This number is taken from the figure below showing the risk of PML after 2 years of Tysabri therapy according to various JCV index levels. We have no information at present to suggest that the manner in which JCV antibody index values vary over time affects the risk of PML. The risk stratification is based on current index value and current duration of therapy. I hope this helps with your decisions. 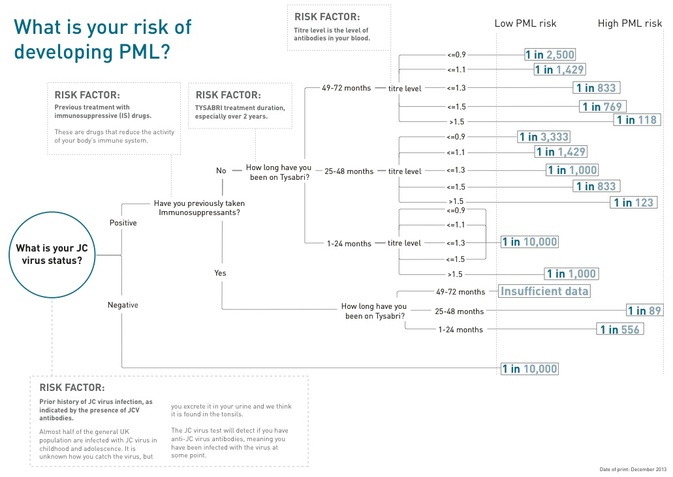 -Rip Kinkel, MD
PLEASE NOTE: The information/opinions on this site should be used as an information resource only. This information does not create any patient-HCP relationship, and should not be used as a substitute for professional diagnosis and treatment. Please consult your health care provider before making any healthcare decisions or for guidance about a specific medical condition. Tysabri can be switched to another MS medication but there are specific issues that must be addressed by you and your physician prior to any switches:
If you go to the search box for this site and type in Tysabri you will see more information that you might be interested in, such as the answer to a question about switching from Tysabri to Tecfidera. -Rip Kinkel, MD PLEASE NOTE: The information/opinions on this site should be used as an information resource only. This information does not create any patient-HCP relationship, and should not be used as a substitute for professional diagnosis and treatment. Please consult your health care provider before making any healthcare decisions or for guidance about a specific medical condition. Question: I am a fan of Beachbody's product Shakeology. I am also a Copaxone user. My issue is that the Shakeology products have the ingredient maca in them. I have used maca in the past but the issue I was running into is that when I would give myself Copaxone injections, I would "bleed out" when I was giving myself the actual injection and I wasn't getting the full amount of Copaxone. In response to this, I had a "mini relapse" and had to go into the hospital for Solumedrol treatment. Is there a way that I can get around this? I really want to take this product but it seems my treatment option is interfering with that. Should I consider Gilenya or another oral treatment instead? Thank you.
Answer: Thanks for your question regarding Maca. I was not familiar with this plant so I had to do a little research. From what I can tell there is little known about the side effects and no mention of bleeding except for some reports of menstrual spotting. Of course, if this has been a reproducible problem for you, Maca may be the cause. That said, it seems like an alternative to Copaxone may be in order for either reason; it makes little difference if the severe relapse was caused by copaxone being ineffective in your case or copaxone leaking out after the injection; in either case it was not working as desired. By the way it is far more likely that the relapse occurred because copaxone is only partially effective in your case. Why not discuss alternatives treatments with your neurologist? Without knowing the details of your case, it is hard to make any specific recommendations. -Dr. Kinkel PLEASE NOTE: The information/opinions on this site should be used as an information resource only. This information does not create any patient-HCP relationship, and should not be used as a substitute for professional diagnosis and treatment. Please consult your health care provider before making any healthcare decisions or for guidance about a specific medical condition. I am currently taking atorvastatin for cholesterol and was wondering if I should switch to simvastatin, considering the latest trials for those of us with SPMS and statins. Is there a difference in the medications?
The answer is no; both atorvastatin (also called Lipitor) and simvastatin (also called Zocor) have been studied in different populations of MS patients with mixed results. Neither statin has definitely been shown to be effective in any MS population, to say nothing about one being more effective than the other. Until phase III studies demonstrate a benefit, it is far too early to recommend any statin therapy to treat MS alone. Those on statin therapy for other reasons (elevated cholesterol, cardiovascular risk) should feel confident in continuing their current statin therapy, if it is working and well tolerated. --Dr. Kinkel PLEASE NOTE: The information/opinions on this site should be used as an information resource only. This information does not create any patient-HCP relationship, and should not be used as a substitute for professional diagnosis and treatment. Please consult your health care provider before making any healthcare decisions or for guidance about a specific medical condition. Trimesta is a branded formulation of Estriol, an estrogen produced in large quantities during pregnancy. It is believed that production of Estriol during pregnancy may be one reason for the decrease in MS disease activity noted in MS patients during the later stages of pregnancy. There are preliminary studies suggesting possible benefits of Estriol in MS, but these studies are far from conclusive. Estriol is not currently marketed for any indication in the united states so it is not even available off label. I am not aware of any phase III trials in progress so the path forward for approval of Estriol in the United States is unclear at this time.
--Dr. Kinkel  Question: I'm new to Tecfidera and have been on it 5 weeks. I seem to be managing my side effects well but it is making me hot. I am taking an aspirin in the morning and it is helping with the flushing but I'm still hot all time, especially at night. How do I regulate my body temperature?
Answer: The first thing you should do if feeling hot is determine if you actually have a temperature. If not then you should see if other medications you are taking could be contributing; these other medications could include anticholinergic drugs like oxybutynin (Ditropan), detrol, vesicle and toviaz used to treat bladder control issues. You may not be able to get rid of them but you may be able to decrease the dose. All of these drugs decrease your ability to sweat and can make you feel hot. If you are not able to get rid of any contributing medications and still feeling hot or flushing, ask your physician about taking a baby aspirin in the morning and another at night if necessary. If this doesn’t work, ask about taking a regular dose of aspirin (325 mg) in the morning and at night. I would suggest taking enteric coated aspirin like ecotrin to avoid hurting your stomach. Hopefully, you will be able to get rid of the aspirin or take just one aspirin after 3 months. Good luck and make sure you check in with your doctors about this problem. --Dr. Kinkel PLEASE NOTE: The information/opinions on this site should be used as an information resource only. This information does not create any patient-HCP relationship, and should not be used as a substitute for professional diagnosis and treatment. Please consult your health care provider before making any healthcare decisions or for guidance about a specific medical condition.  The easy answer to your question is no, I do not think that dietary manipulation is an effective way to manage your MS. But I would give the same response if asked if medications were an effective way to manage Multiple Sclerosis. MS, like many chronic conditions, can not be managed with any single remedy since the goals of treatment are diverse. I suppose if someone discovered a cure for the condition, you would only need to apply this cure and other treatments would lose their significance. Until this time any effective management strategy must reduce inflammatory responses in the central nervous system, protect cells from ongoing stress and neurodegeneration and assist in remyelination and regeneration. There is no dietary manipulation able to accomplish any of these goals by itself although dietary manipulation may play a role in the treatment process. As to which diet is most effective, no one knows the answer.
-Dr. Kinkel Question from an MS Patient:
Is Rituxan an effective treatment for SPMS? What are the benefits or disadvantages? i.e. pros & cons etc. Are there any life-threatening side effects? Would you consider this is a good drug to treat SPMS long term? Do you feel the drug can cause complications-manifest other diseases or illnesses? Are there any results from clinical trials conducted using Rituxan published? Rituxan (Rituximab) is a chimeric monoclonal antibody that is currently approved for the treatment of two forms of cancer (CD20 positive Non Hodgkin’s Lymphoma (NHL) and chronic lymphocytic leukemia (CLL)) and two immune medicated disorders (moderate to severe rheumatoid arthritis and Wegener’s granulomatosis). It was first approved in 1997 and has been widely used off label to treat a number of rare immune medicated conditions, including neuromyelitis optics (NMO), often with dramatic success. In fact is it currently considered the first line treatment for NMO in many centers around the world. It binds to a protein expressed on the surface of B Cells called CD20 and causes complement mediated lysis of these cells lasting for variable periods of time depending on the dose administered. The mechanism of action in MS is unclear; B cells clearly play a role in the inflammatory response in MS and their elimination seems to benefit many patients. What is unknown is the exact role played by the B cell; for instance some believe the B cell only becomes a problem in MS when co-infected with Epstein Barr Virus. Studies of Rituximab in the treatment of relapsing or progressive forms of MS have been few, yet it remains a key treatment option by many MS specialists for certain situations; namely, as an induction therapy for patients with an aggressive onset to their condition, as ongoing treatment in relapsing patients not responsive to other therapies including tysabri or in patients rapidly transitioning to secondary progressive MS despite other available treatment options. Why would a drug not even approved by the FDA be considered such an important treatment option by MS specialists? First, those studies that have been done in relapsing forms of MS demonstrate rather dramatic benefits that persist for 6 to 12 months after treatment. MS specialists using the drug in practice report similar benefits in their patients. Studies in progressive forms of MS have reported mixed results which can be expected given the challenges of treating MS at this stage of the disease. The large phase III study by Genentech in primary progressive MS was a negative study when the entire study population was considered in the analysis. When considering only those patients under the age of 51, those patients with gadolinium enhancing lesions at the beginning of the study or patients with both features, rituximab given every 6 months for 4 courses of treatment significant reduced the rate of sustained disability progression. A small retrospective analysis of 25 secondary progressive MS patients treated with rituximab every 6 months at the University of Massachusetts in Worcester reported that 84% of patients stabilized or improved while on treatment. Rituximab is generally safe in most MS patients. The most common side effects are caused by infusion reactions which decrease over time and can be further decreased by administering corticosteroids prior to the infusion. There is also a slight increase in serious infections, though these are treatable. Progressive Multifocal Leukoencephalopathy (PML) has been reported but does not appear as frequently as in Tysabri treated patients. What is unknown are the long term consequences of treatment with Rituximab and the most appropriate dose and dosing interval. Most current dosing regimens are based on the very high doses used to treat cancers, yet we were able to achieve a very good response in relapsing patients given 1/20th of this dose (100 mg) every 6 months for over 3 years of continuous treatment. Further studies of rituximab are not likely to occur since there is no further patent protection. There are several other monoclonal antibodies in MS clinical trials that target CD20 and delete B cells including ocrelizumab and ofatumumab. Whether these newer treatments offer improvements in safety or efficacy in comparison to rituximab is unclear at this time. --Dr. Kinkel PLEASE NOTE: The medical information on this site is provided as an information resource only, and is not to be used or relied on for any diagnostic or treatment purposes. This information does not create any patient-physician relationship, and should not be used as a substitute for professional diagnosis and treatment. Please consult your health care provider before making any healthcare decisions or for guidance about a specific medical condition. |
PLEASE NOTE: This information/opinions on this site should be used as an information source only. This information does not create any patient-HCP relationship, and should not be used as a substitute for professional diagnosis and treatment. Please consult your health care provider before making any healthcare decisions or for guidance about a specific medical condition.
Archives
March 2024
Categories
All
|
|
|
© 2023 HealthCare Journey, LLC. All Rights Reserved. HealthCare Journey™ is a trademark of HealthCare Journey, LLC |
|
 RSS Feed
RSS Feed