|
A Modern definition of MS Disease Types useful for Therapeutic decisions March 23, 2016 I am often asked how MS specialists characterize the disease course and use this information for making treatment decisions. Most of the patients I meet want to know if they have relapsing remitting, secondary progressive, primary progressive or progressive relapsing MS. These are old classification terms based only on clinical features and then to create confusion without helping us with management decisions. The table below shows a classification system that we developed initially during the CHAMPIONS study and refined over time as we developed better tools to monitor. 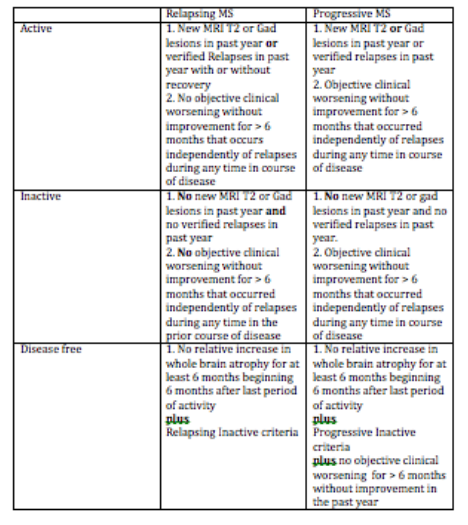 MS activity with MR imaging. This classification eliminates the older terminology and concentrates on defining inflammatory activity as the primary driver of treatment decisions and cessation of disease progression and brain atrophy (both linked concepts) as the ultimate goal of treatment (disease free). This criterion does not incorporate known risk factors for disease activity and worsening which we use concurrently to determine the most appropriate disease modifying therapy. In other words not all relapsing active or progressive active patients are the same in terms of treatment decisions. For instance, those people with MS who experience severe or frequent relapses with incomplete recovery require treatment with highly active DMTs whereas those early in the course of the disease with mild infrequent relapses and a low MRI burden of disease do not require highly active DMTs. The newer classification begins by characterizing MS as Relapsing or Progressive. This is entirely determined by clinical features. The course is then qualified as active or inactive based on a combination of clinical and MRI features. Relapsing patients have periodic, often rare relapses, with little if any continuous worsening of their condition between relapses that can be measured. Relapsing patients also tend to experience new T2 or Gad-enhancing lesions even in the absence of clinical relapses. We now combine clinical relapses and new MRI lesions as our definition of inflammatory activity over a given interval of time. Progressive patients slowly worsen over periods in excess of 6 months in a way that we can measure in the clinic, although they often spontaneously experience relatively long periods of clinical stability even without treatment. Progressive patients may also experience relapses (see above for activity definition) and new MRI lesions, particularly in the early course of the disease. These progressive active patients are excellent candidates for disease modifying therapy (DMT), especially newer highly active DMTs. To be completely disease free you must meet the additional criteria of experiencing a rate of brain atrophy no greater than healthy controls following recovery from a period of activity. This is a high standard to achieve by treating people with most current DMTs and, as a result, most centers do not currently quantify brain volumes on their patients. This is rapidly changing and will be an important treatment goal in the future Symptoms of progressive disease can vary but tend to involve previous areas of involvement by relapses or MRI activity. For instance, those people who tend to experience weakness on the right side during relapses have a greater tendency to experience slowly worsening right sided weakness as a sign of progressive disease and those with a larger cerebral burden of disease with early cognitive difficulty often experience a decline in cognition as a sign of progressive disease. The actual symptoms vary tremendously from one patient to another. The time course for these stages in also highly variable; Relapsing disease tends to last for 5-25 years and progressive disease tends to begin 0 to 25 years after onset. As mentioned above we use various risk factors to determine a persons risk of experience more aggressive disease in the near future. These risk factors are exclusively clinical and MRI measures at present but will likely incorporate other biomarkers in the near future. We tend to use disease-modifying therapies (DMTs) in those patients meeting activity criteria, whether progressive or relapsing in type. Those with long standing progressive disease without any activity do not respond as well to any of our current therapies. Revere (Rip) Kinkel MD Director of the Multiple Sclerosis Program Professor of Clinical Neurosciences University of California San Diego
Patricia Smith
6/16/2016 08:04:30 am
why do you use mri results for everyone but me? you nave always indicated that you didn't rely on that information much.
Dr Kinkel
6/23/2016 07:33:08 am
Routinely repeating MRI scans every year (or more often) using standard techniques for acquiring and analyzing the scans is not useful in most older patients (generally > age 55) with longer duration of disease (generally > 10 years). For this group of patients, the MRI scans must be acquired using 3 Dimensional Imaging sequences and analyzed with special computer algorithms. This is not available at most centers, although it is available at UCSD. Comments are closed.
|
DISCLAIMER:
The medical information and opinions on this site are provided as an information resource only, and are not to be used or relied on for any diagnostic or treatment purposes. The information and opinions expressed do not create any patient-physician relationship, and should not be used as a substitute for professional diagnosis and treatment. Please consult your health care provider before making any healthcare decisions or for guidance about a specific medical condition. Archives
January 2020
Categories
All
|
||
- Home
- About Us
- Virtual MS Center
- News & Resources
- Seminar Registration
- Health & Wellness
- Blogs
- About MS
-
Symptoms
- Balance and Walking Issues
- Breathing/Respiratory
- Bowel Dysfunction
- Cognitive Dysfunction
- Crying/Laughing Uncontrollably (PBA)
- Depression and Anxiety
- Dizziness/Vertigo
- Dysphagia
- Fatigue
- Foot Drop
- Hearing or Smell or Taste Changes
- Heat Sensitivity
- Leg Weakness
- Loss of Hand Dexterity and Coordination
- Memory and Mutliple Sclerosis
- Migraines
- Numbness/Tingling/Altered Sensation
- Nystagmus and Oscillopsia
- Pain
- Sexual Dysfunction
- Sleep Issues
- Spasticity/Spasms/Cramps
- Speech/Swallowing
- Urination/Bowel Problems
- Vision
- MS Clinics
- MS Topics
- Register With Us
- Terms of Use/Privacy/HIPAA
- MS HealthCare Journey
 RSS Feed
RSS Feed