|
ECTRIMS Meeting Boston MA
September 10,2014 As I return to Boston for the start of the largest international MS meeting of the year, my thoughts have turned to the many wonderful resources that were and still are available to patients and their families in this area. From the many comprehensive MS Centers to the outstanding universities and research labs, Boston is truly an amazing place for people with MS. But one additional Boston area resource that is available in very few other locations around the country and often helpful to the many women with MS is a store in Brookline called Good Vibrations. As the name suggests, some may call this a sex shop but it is unique among enterprises of this nature with it’s attention to the needs of women (as well as LGST couples) and it’s focus on education. The staff are provided with extensive training and I’ve never heard of customers feeling uncomfortable with either the location or the store atmosphere. I’ve even heard of mothers and daughters visiting the shop together. Their emphasis on education is remarkable with a staff sexologist, Carol Queen PhD, available. In a world where the management of sexual dysfunction seems confined to improving erections in men, and medical doctors are still of little help to women with sexual dysfunction, it is good to know that there are resources available to women with these problem. There are Good Vibration stores also available in San Francisco, California although I have no personal knowledge of these stores. If you know of similar resources available in your community, please comment so we can post this information for other patients and families. So with the ECTRIMS meeting now underway, take some time out to visit Good Vibrations if you live in the area and you think this may help. After all, a healthy sex life has been shown to benefit fatigue, pain, sleep disruption, mood and well being. I will now return to the meeting and provide updates later this week or next week on new management strategies that may be of benefit to you now or in the near future. Good Vibrations 308 Harvard St Suite A Brookline, MA 02446 goodvibes.com -Rip Kinkel, MD  Here is My Question:
I have RRMS. I don't want to take medications. What's the biggest risk if I don't? Answer: Disease modifying therapies (DMTs) for MS are 1) expensive, 2) associated with a variety of side effects and potential safety risks, and 3) are partially effective. With this understanding, your question is one I hear frequently in clinic. The major risk of deferring DMT for relapsing-remitting MS is an increased likelihood of clinical relapses in the future that can disrupt your day-to-day function, and short- and long-term disability. Let me explain… We have a great deal of natural history data on MS (this is information on the average experience of patients with MS who were not exposed to therapy). This information is available to us because it wasn’t until the mid-1990’s that we had our first approved DMT for clinical use. What we have learned is that patients with early and frequent clinical relapses are at a higher risk of developing walking disability (for instance, the average individual with greater than 5 clinical attacks in the first 2 years of MS will need a cane to walk by 6 to 7 years into their disease course; while the average patient with 0 or 1 clinical attack will need a cane by the 20 year mark). We have also learned that the initial MRI brain scan after the first clinic event of MS can tell us about the likelihood of disability in the future—the more scars of MS that are seen on this first scan, the greater the probability for disability sooner rather than later. Keep in mind that these numbers reflect MS patients who did not have DMT options. At the time of this blog post, we have ten FDA-approved DMTs, with more being reviewed. In nearly every case, these therapies have repeatedly shown effectiveness in 3 main measurements: 1) less clinical relapses or attacks compared to placebo, 2) reduced number of new, enlarging, or enhancing scars on the brain MRI scan, and 3) a reduction is short-term disability compared to placebo. Critics have long pointed out that the DMTs are not cures, are expensive, have variable safety risks, and have not been proven to make a difference in the long-term. While it is true that all DMTs are partially effective—meaning that the data does not show that they cut down new relapses, MRI lesions, and disability by 100%—they have recently demonstrated effectiveness in the long-term. In 2012, a paper was published in the journal Neurology that presented long term follow-up data on the first approved DMT called betaseron. This 21-year study followed the originally randomized study participants (an early treatment group that was randomized to betaseron from the beginning, and a late treatment group that comprised individuals that were originally randomized to placebo but were given the opportunity to take betaseron after the initial clinical trial ended 3 years later). This paper showed that there were more people alive from the early treatment group 21 years later compared to those in the late treatment group. You can read more about this at http://msj.sagepub.com/content/19/5/522.full. This study confirmed our suspicions that DMT does help in the long term and does underscore the need to treat early rather than waiting—because there appears to be a window of opportunity to alter the course of the disease for the better. Many of the barriers to initiating a DMT for relapsing-remitting MS patients have been removed. There are financial and co-pay assistance programs in place to make DMTs affordable for patients, risk mitigating protocols for DMTs, and experienced MS clinicians that can help you in choosing a reasonable DMT that can fit your goals and lifestyle, and outline a plan to make sure the medication is doing what we expect it to do and make it tolerable for the patient. While the majority of my patients ultimately decide to start a DMT after considering this information, some choose to defer treatment. That is certainly each individual’s prerogative. Before making the decision, everyone should recognize the fact that we do not yet have a therapy that can reverse or repair tissue damage already incurred due to MS inflammation, nor do we have a therapy at the moment that reverses sustained disability. What we are left with are DMTs whose purpose is to get in front of the disease and impact it for the better, and hopefully avoid significant disability in the future. -ASN  Problems with thinking or performing normal daily cognitive tasks are a hallmark of Multiple Sclerosis and often grouped with fatigue and depression (as well as anxiety) as the main hidden symptoms of the disease. In fact this constellation of symptoms, reported in over 50 % of newly diagnosed patients, often dominates the lives of people with MS early in the course of the disease when physical manifestations are less apparent and the amount of involvement of the nervous system is relatively limited.
It should therefore come as no surprise that there is often little relationship between the extent of visible white matter involvement on MRI scans and the presence of these hidden symptoms. Given the interrelationship between fatigue, depression (often with sleep disruption) and mild cognitive impairment it has been hypothesized that all three symptoms may be intricately linked early in the course of the disease through some common mechanism or pathway. In fact successful management of perceived cognitive impairment early in the disease requires a multidisciplinary approach directed at the impact of mood disorders, sleep disruption and fatigue with or without compensatory strategies to help with specific cognitive tasks. Treating only one aspect of this triad is less likely to be successful, as researchers have discovered in clinical trials of drugs to treat fatigue, where patients reported improved fatigue but no change in cognitive performance. But what are these cognitive problems reported by patients with MS and why are they so difficult for others to recognize? In its mildest form people with MS report forgetfulness and slowing of thought processes often with word finding difficulty and easy distractibility. These symptoms are identical to those reported by people with isolated chronic fatigue syndrome and depression, thus supporting the connection discussed previously. It is very rare for MS to create obvious problems with language, the ability to carry out common learned tasks (combing one’s hair or knowing how to use eating utensils), or limit awareness of one’s environment to the extent that is typical of dementing illnesses like Alzheimer’s disease. Some people with MS become even more gregarious and outspoken with time (think, “no filter”), again leading those around them to often fail to recognize the worsening problems with cognition and incorrectly attribute the actions of the patient to willful misbehavior or a personality problem. The intrusion of crying spells, difficulty controlling smiling or laughing or emotional fluctuations can further lead people to believe that the problem is solely a reflection of depression or another mood disorder, even though there is no other evidence to support a diagnosis of mood disorder and the behavior is not linked to any particular environment clue or stimulus. Thankfully, these problems with emotional lability do not typically occur early in the course of the disease, if at all. But even early in the course of the disease, learning new information (visually or verbally or both) can be enough of a problem to interfere with school activities or learning a new job task, whereas old well learned tasks remain relatively unaffected. Once a patient loses the ability to sort and manipulate information, inhibit incorrect responses and develop a cognitive plan to an degree that impairs their ability to execute multistep tasks (this is reason it is called executive dysfunction), it is often very difficult for people with MS to remain employed even with compensatory strategies. This often happens well before an individual has lost enough physical function to require disability solely on the basis of their physical problems, and is the main reason that cognitive impairment is the main cause of loss of employment in MS. The lack of supporting documentation of their cognitive impairment in the form of specific cognitive testing, and the failure of families, employers and physicians to recognize the impact of these deficits on everyday behavior and the ability to perform work related tasks is the main reason for divorce, job terminations and failure to obtain disability. This in turn creates greater stress on patients, caregivers and other family members in a vicious cycle that is very hard to halt or reverse. But are all people with MS destined to decline in such a dismal manner or do certain features or characteristic of one’s environment or one’s disease predict worse outcomes and possibly offer an opportunity to intervene to improve outcomes? This is a topic that I have discussed in several previous blogs and is very pertinent to any discussion of cognitive impairment and it’s treatment. First, there are certain individual characteristics that unfortunately are not amendable to modification. Foremost among these are the susceptibility genes we inherit that may affect disease severity, and early childhood enrichment, nurturing and education, collectively referred to as, “passive cognitive reserve”. Many studies in MS and other degenerative disorders suggest that greater childhood enrichment and education is protective against cognitive decline from a number of diseases later in life. Thankfully, many studies also suggest that “active cognitive reserve”, or ongoing learning and development of new skills in adult life is also protective and the reason so many experts advocate memory games and the acquisition of new skills in older adults. This should form of the core of any treatment strategy to prevent cognitive decline. What about specific disease characteristics associated with a more rapid decline in the physical function of MS patients? Remember, cognitive impairment is like any other manifestation of MS; features associated with a more aggressive disease course and rapid physical decline tend to be associated with more rapid and significant declines in cognition. Since men and African Americans tend to have more severe problems with MS, it stands to reason and is supported by data that they also tend to have more problems with cognition as the disease worsens. Similarly, greater MRI white matter involvement at onset of the disease or developing within the first few years of the disease tends to be associated with greater development of cognitive impairment over time. An even better predictor of cognitive impairment is the degree of brain atrophy or the rate at which brain volume declines over time. Therefore, treatments that are more effective at preventing the disease from getting worse, as defined by MRI and physical examination, should have a similar benefit on preventing or slowing the development of cognitive impairment over time. This in fact has been demonstrated in clinical trials of disease modifying therapies beginning with the seminal study of Avonex for relapsing MS. There is every reason to suspect that disease-modifying therapies that significantly affect the course of the disease should lessen cognitive impairment, although not all clinical trials include adequate assessments of cognition to test this hypothesis. Therefore, the most important treatment for cognitive impairment, and the treatment supported the most by clinical research, is prevention of further worsening with effective disease modifying therapies. What is not known is whether the benefits of disease modifying therapies accrue to patients in both early and later stages of the disease or whether the benefits are enhanced in either group by cognitive enrichment and learning programs although there it is probably a good bet that both treatment strategies are required. What other features should be considered in the assessment and management of cognitive impairment? As noted previously, the assessment and management of mood disorders and fatigue are essential if one is to have a significant impact on the manifestations of cognitive impairment. This is true at all stages of the disease. Equally important is the discontinuation of potentially offending medications that are not required and contribute to cognitive complaints. The list of medications that may worsen cognition is almost endless but is dominated by narcotics (eg Percocet, vicodin etc), sleep aides, benzodiazepines (eg include valium, lorazepam), alcohol and marijuana. To be sure, many people require these medications but there are many with no need for them or with a different need that requires a less harmful treatment. Lastly, it is exceedingly important to eliminate other potential disorders that may worsen cognitive impairment in people with MS. These conditions, many of which are more common in people with MS than the general population, include thyroid disorders, sleep disorders, (sleep apnea and other primary or secondary sleep disorders) and Vitamin deficiency, particularly B12 deficiency. Periodic worsening of cognitive is common later in the disease and frequently associated with undetected infections (UTI) or the development of new medical problems (heart disease, COPD). What about specific pharmacologic treatment of cognitive impairment? Unfortunately, specific treatment of cognitive dysfunction in MS patients with drugs used to treatment other memory disorders like Alzheimer’s disease has not been beneficial; these treatments include Donepezil, Rivastigmine and Memantine. Furthermore, all of these treatments may create unacceptable side effects. Ginko Biloba has a long history of use for this symptom but controlled studies suggest no significant benefits in MS or significant side effects. As mentioned previously, treatments meant to ameliorate fatigue, such as amantadine and modafinil, may benefit fatigue and excessive daytime sleepiness, but alone will not generally improve cognition. This does not mean the drugs used for fatigue do not play an important role in multidisciplinary management of cognitive impairment. What is the best approach to cognitive impairment in MS at this point in time?
-Rip Kinkel, MD  Recent changes in the healthcare system and medical advancements offer the hope of more effective management of complex chronic diseases such as Multiple Sclerosis; but many patients and providers are undeniably frustrated by the day to day reality of these changes, whether it be the need to switch insurance plans and providers, the larger copays and deductibles, the increased requirements for prior authorizations, the increased documentation requirements to receive payment, the shorter times available for visits and the never ending announcements of the next cure or advancement that arrives too late or not at all.
Now that we have all expressed our frustration and got it out of systems, I’m here to tell you it is time to stop complaining and focus on managing those things we can control. Change is always hard and we need to find constructive ways to manage change and harness the benefits of common advancements like the electronic medical record (EMR) systems required under the Affordable Care Act, better known as Obamacare. Let’s start with how to maximize the benefits of a typical doctor-patient visit. For years I’ve watched people arrive for their visits unprepared. A doctor arriving unprepared is also common, but since your only recourse is to get rid of the doctor, let’s focus on the patient side of the equation. How many times have I listened and tried to understand the chronology and characteristics of a patient’s problem in the privacy of the exam room while they discuss and sometimes argued with various relatives or friends about the facts of their case? I have a secret for you; these interactions between patients and those who accompany them are often more instructive to the doctor than the medical facts, but I digress. People spend a great deal of time keeping their resume and financial records up to date but how many actually keep their medical records up to date. When I ask a patient for discrete information like the start and stop date of a prescribed medication or a hospitalization their answers are often incorrect by years. I know what you’re thinking because I’ve heard it from my own family members; many of you believe that because the doctor or nurse or some other health care professional is writing everything down that all of your history and data is carefully preserved and shared among all providers. Well it isn’t. Many also believe that medical institutions share records and results. Perhaps in the future, this will be the case, but at present we are limited by an extensive series of privacy laws called the Health Insurance Portability and Privacy Act of 1996 (HIPAA). As with most regulations, HIPAA is a great idea at face value but the funding to comply with HIPAA is not available and information flow actually is slower under HIPAA because of the security requirements and medico legal concerns. So the bottom line is that even if your health information is carefully recorded (a big if) it is not shared easily or willingly. And even if it was carefully recorded it is your responsibility to make sure the information is accurate and available for appointments. So the main step you must take to get the most out of your interactions with the health care system is to take control and responsibility for your own health information. Even the best electronic medical system may crash on the day of your visit, so you might as well have a back up ready. I am going to outline the main things you and your doctors need to do to improve visits. In subsequent blogs and additions to this web site we will implement and provide some of these features for you; then you can decide with whom you want to share your medical information at any time by a simple click of a button. All that is required is a computer and Internet access. A scanner is useful for document storage. Once information is inputted either a smartphone or tablet app can be created to provide ongoing or updated information. 1. If your health care provider uses an electronic medical record (EMR) system use it to its full potential. Ask to review the information already entered and make corrections as necessary. This is something useful to do while waiting for the doctor and is actually your right under the HIPAA regulations. Reviewing your information is a necessary step since doctors often repeat information in your chart to save time and perpetuate mistakes. For instance, I had a patient that was admitted years ago for abdominal pain eventually diagnosed with severe viral gastroenteritis after discharge. The doctors were worried about pancreatitis on admission but never removed this diagnosis from his record. All subsequent notes list this man as having a past medical history of pancreatitis. Most electronic medical record systems also allow you to communicate with your doctor and his facility through a secure Internet portal. At Beth Israel Deaconess Medical Center this was called patientsite and on Epic based systems like UCSD this is called MyChart. This gives you access to almost all your medical information and sometimes gives you access to your doctors’ notes. You can ask questions, see results of testing and copy it for your records, and refill medications and schedule appointments through these systems without waiting on telephone hold. If these systems are available to you, sign up and use them. But remember, if you are seeing doctors at two different institutions, their EMRs will not communicate yet and may not for a long time. This is one advantage of staying within one system. In the future a system of Accountable Care Organizations (ACO) will formally create networks of health systems that shares your medical information and are accountable for your care. The different ACOs will not necessarily communicate with one another but communication among the health systems within each ACO will be improved. 2. You need to keep a medical history on your computer and bring a print out or your computer or tablet to visits. If you’ve completed step 1 above, then this will not be necessary once you establish care with a doctor who uses an EMR system. The average MS patient sees a new doctor every 3 years so it is best to be prepared for these new interactions. Hopefully, this information will not be required after your initial visit with your new doctor, but it is better to be safe than sorry. Just as there are templates for resumes online, there are many templates for personal medical histories as well. We will be posting a medical history form for MS patients soon and provide a secure online site to update this information 3. Keep copies of test results in a notebook or better yet, scan them into your health record on your computer. Make sure the file name identifies the scanned document. For instance an MRI report could be assigned a file name, MRI_Brain_3.13.14, to indicate an MRI of the brain on March 13th, 2014. Remember, if a test is done at your doctor’s facility it will appear on his EMR system, but if you do it closer to home or in another facility, chances are your doctor will never see the results unless you make sure he or she gets them. Think of this when you are in a hurry to leave after an appointment and decide to skip the blood draw lab and get tested closer to home. It becomes your responsibility to make sure somebody actually sees the result. 4. Medications are a special part of your health record. Federal requirements for certain payments to doctors require health care providers to use EMRs to prescribe and record medications electronically. Gone are the days of doctors scribbling illegible prescriptions on paper pads and handing them to patients. The only exception is controlled substances, which still cannot be sent electronically; this includes narcotics (vicodin, Percocet, Darvocet morphine etc), benzodiazepines (diazepam, lorazepam etc) and stimulants (methylphenidate, Adderall etc). Different states have slightly different requirements for controlled substance prescriptions. If you have a doctor who uses an EMR, never leave without a corrected and updated list of your medications for your records. Whenever you start or stop a medication you should add these dates to your medical history (# 2) with the reason for starting or stopping the medication clearly stated. If you are seeing a doctor for the first time and do not have a list of your medications, the next best thing is to bring all the bottles of your medications to your appointment. 5. MRIs are a very special part of your medical record and one that is often not available when needed at the time of a visit. MRIs help establish or confirm your diagnosis and form the basis of many treatment decisions. Unfortunately, insurers sometimes require that you obtain an MRI outside of your doctor’s institution or you end up choosing another MRI facility because is more convenient or less expensive or both. There are two problems with this system. First, these outside MRIs will usually not be available to your doctor unless you bring an electronic copy on a CD. When the MRI facility tells you they will send a copy to your doctor, they are lying. The only thing they will send is a useless report. They may say they will send a CD but this rarely occurs. Make sure you do not leave without a CD of your MRI in your hands to take to you doctor or to upload for your doctor (see below). The second problem is that an outside facility may not perform the type of MRI needed for your situation even if asked. It is my opinion that all Brain MRIs on MS patients should be acquired using both 3D FLAIR and 3D T1 sequences but these are rarely done in practice. In the near future it will be important for you and your doctor to make sure that the MRI facility is willing to do the correct image acquisition before agreeing to let the facility do your MRI. Why is this important? Soon you will be able to take your MRI on a CD or directly from the radiology center and upload it to a CLOUD server that will perform quantitative analysis that allows your doctor to make more accurate and timely treatment decisions. Stay tuned as we will be posting access to one of these servers on this website in the near future. 6. Now it is time to talk about the actual visit with your health care provider; you’re all prepared and probably nervous. Broadly speaking there are 3 types of patients I encounter; those doing their best to convince me that they have serious problems and want help, those trying to perform at their best to convince me that everything is all right so as to get a good report and those somewhere in the middle. Each type of patient require a different approach but, as with politics, it is usually best to remain somewhere in the middle. By this I mean it is important to analyze information carefully, recognize both the positive and the negative during your visits and take a measured approach focused on achievable goals. How do you get there?
Remember, more accurate and readily available information can only improve the quality of your healthcare. -Rip Kinkel, MD  Exercise is probably the most important therapy for MS and serves as the platform for all other treatment modalities.
This being said, some people have difficulty initiating and continuing exercise programs for reasons both related and unrelated to their MS. Since the perceived barriers to exercise are almost too numerous to list, I find it far easier to list some core principles to follow:
I am often asked a variation on the same question, so I thought it best to write a blog that addresses the entire concept. The question is often phrased in one of the following ways:
The theme of each question is identical; why after years of stability would someone with MS slowly get worse? There are, of course, several possibilities; it is most important for an individual with this concern to consult with an MS specialist or neurologist to determine the most likely reason for this delayed worsening after many decades of stability. One common cause is that the person has developed a new problem unrelated to MS, such as cervical spondylosis; this is a form of arthritis that can cause compression of the spinal cord with progressive walking difficulties often with stiffness and limited range of motion in the neck and neck pain that migrates into one or both arms. Many other reasons for delayed onset of neurological symptoms in an MS patient exist and require an evaluation to sort out. Another possibility is that the individual is developing secondary progressive MS; in some MS Clinics when this occurs after a single attack, the MS course is referred to as, “single attack onset progressive MS”. Determining if this is the cause of the worsening can be difficult and often requires years of observation for the clinician to be sure. More commonly, a person develops secondary progressive disease after experiencing more typical relapsing remitting MS earlier in life. The years of relatively stability without relapses before the onset of progressive worsening is not unusual, as relapses tend to get rare as you get older. The real question is what is happening during those years or even decades of stability? To answer this question in a manner that is easier to visualize I created the figure to go along with this blog. 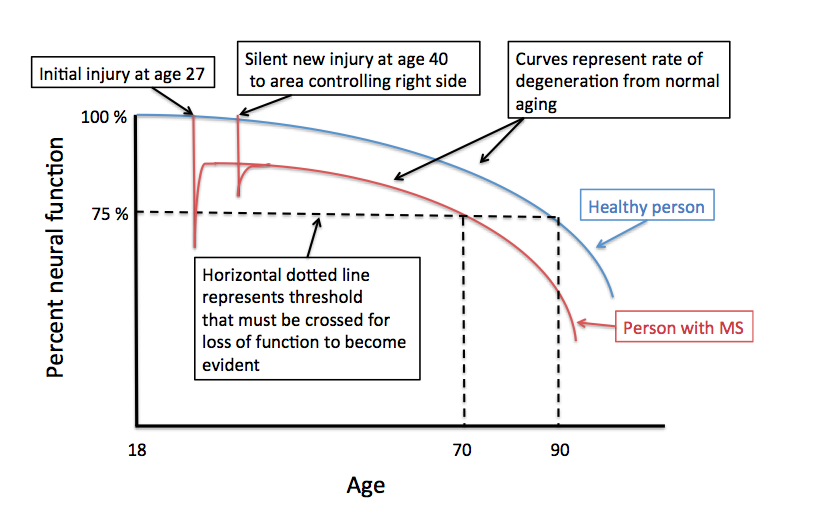 The Y-axis represents percent neural function and the X-axis is age. The figure begins at age 18 after the conclusion of normal development; at this time you should have 100% neural function assuming no injuries during development and adequate enrichment (diet, exercise, education, nurturing). The blue curve represents the gradual decline in neural function with age. This decline is probably not linear and is certainly affected by many life events as well as illnesses and chronic diseases.
Eventually, a normal healthy individual crosses a certain threshold of declining neural function, represented by the horizontal dashed line, and is no longer able to compensate well. In the example provided this occurs after the age of 90. I’ve labeled the threshold as 75% of normal neural function, but this is an arbitrary percentage; the threshold may be lower or higher or variable by region depending on a number of factors including physical and cognitive enrichment during development and ongoing physical, cognitive and social activity throughout adult life. We refer to these factors as passive and active neuronal reserve, respectively. Most studies indicate that active neuronal reserves, or your physical, cognitive and social activities in adulthood, are the most important in determining the affects of normal aging and the outcome from chronic neurologic disease like MS. The red curve represents a theoretical MS patient who experiences their first neurological symptoms at the age of 27; let’s say this causes left sided weakness. At the time of this attack (or exacerbation) the area of the nervous system responsible for the left sided weakness is temporarily injured and neural function declines below the 75 % threshold. This causes the patient to experience the behavioral manifestation of this decline in neural function (e.g. left sided weakness). In the example provided complete recovery of this behavioral manifestation of the neural injury (the left sided weakness) occurs even though the area is no longer able to provide the same level of neural function as a normal individual (i.e. the red line does not return to the blue line). This recovery occurs because of partial injury at onset, resolution of inflammation, remyelination and repair and neural plasticity (other areas of the brain taking over the behavioral function of the injured area or new connections forming from the injured area or both). In this same example the patient is remarkably stable and does not experience any further injury from MS until the age of 40. This time the injury does not cross the threshold and no symptoms occur, even though the area involved normally controls right-sided strength. An MRI may or may not show a new area of involvement and tissue recovery occurs once again. As we now trace out the red line while the person ages, we notice that the line crosses the 75 % threshold at an earlier age (age 70) than the healthy person represented by the blue line (age 90). At this age the MS patient can expect their left sided weakness to return and they will now slowly develop new right-sided weakness from the prior silent injury at the age of 40. How can this be prevented? One way is to prevent further injury from MS by using effective disease modifying therapies. The best way to shift the threshold line lower and therefore prevent the onset of declining neural function with age is to increase your active neuronal reserve. This is done by remaining healthy and actively involved with life through regular physical exercise, cognitive activity -particularly learning new skills- and remaining engaged socially. Now you know why I continually harp on the importance of remaining active in all these domains of life. Rip Kinkel, MD It is time to start talking about MS prevention and treat your relatives...
We’ve known since the 1980’s that the risk of MS among first-degree relatives (a genetically related child or sibling of a person with MS) is 2-5%. Initially, we did not know if there were factors, preventable or not, conferring either a higher or lower risk of developing MS. Because of this we tended to reassure these families with the knowledge that at least 95% of their offspring or siblings would not develop MS (excluding identical twins). Accumulating evidence of genetic and environment risk factors for MS over the past 20 years strongly suggests that the risk of MS in certain family members may be considerably higher than the quoted 2-5%. For this reason and the mounting evidence that the incidence of MS may be increasing in some population groups, we believe it is time to begin talking about MS prevention. As a starting point, it is important to remember that the 2-5% risk of MS among first-degree relatives of MS patients is an overall average risk, not a particular individual’s risk. To understand this better let’s consider an example of a theoretical disease that occurs in 1 out of 1000 people or 0.1% of the population. Overtime we may learn that 1 out of 100 first-degree relatives get the disease or 1%. This is useful information (i.e. a 10 fold increased risk over the general population) but perhaps not actionable. If we then learn that 25% of first degree relatives with a particular genotype and exposure to a particular virus develop the disease and only 0.2% of the first degree relatives without this profile develop the disease, you now have information that can be acted upon. The situation with MS is approaching this level of understanding. To know the individual risk of MS in a first degree relative requires knowledge of the family member affected, when they were affected (younger or older age), environmental risk factors (read below) at different exposure ages, genetic background, the incidence of MS in the area the individual grew up in, and possibly an assessment of particular biomarkers (typically from a test done on a sample of blood, urine or spinal fluid) measured over time. Knowing this information can allow clinicians to develop a risk profile for an individual. In fact, Dr. Philip De Jager and his colleagues at Harvard are working on the development of this type of platform. Based on the profile of an individual family member, it is likely that their risk of developing MS could vary from < 1% to as high as 25%. The actions this individual or their parents would be willing to take to minimize this risk of MS will obviously depend on both the risk of developing MS and, more importantly, the risk that their MS would be particularly severe. Future studies will hopefully allow us to assess both risks. But what can we do at present without this multidimensional data to guide us? Since we cannot do anything at present about inherited risks, it is important to focus on modifiable risk factors. It is our opinion that there is enough information currently available to help decrease the risk of developing MS among first-degree relatives by simply managing the following known risk factors: 1. There is significant epidemiological evidence that Vitamin D deficiency is associated with a higher risk of developing MS. This risk may begin even before birth based on evidence that MS is more common among children born in winter months when UV light exposure and 25-hydroxy vitamin D levels (25(OH)D) are at their lowest. There is also significant evidence that vitamin D3 supplements in pregnant woman, young children, adolescents and adults are safe in doses much higher than currently recommended by the institute of medicine (IOM) or American College of Gynecology and Obstetrics (ACOG). Although there are no controlled studies demonstrating that vitamin D3 supplements decrease the risk of MS or the level of 25(OH)D (this is what doctors measure in the blood when they check your Vitamin D level ) that must be achieved to decrease this risk, we do have some information to guide us. First, a woman planning pregnancy or pregnant with an unborn child that has a first degree relative with MS (either the mother herself, the father or a sibling of the unborn child has multiple sclerosis) and a 25(OH)D level less than 20 ng/ml (or 50nmol/lt) is Vitamin D deficient by all criteria and requires high dose supplementation with at least 50,000 IU per week of vitamin D3 or equivalent daily dosing (5,000 IU vitamin D3 or greater per day) with a goal of rapidly achieving a 25(OH) D level > 40 ng/ml (100 nmol/lt). We recommend that pregnant woman with levels between 20 and 40 ng/ml (50 to 100 nmoles/lt), supplement with 4,000 to 6,000 IU per day of vitamin D3 to achieve these same 25 (OH) D levels (greater than 40 ng/ml (or greater than 100 nmol/lt) ) although many will require doses over 6,000 IU to achieve these vitamin D levels. Those with levels greater than 40 ng/ml (100 nmols/lt) prior to supplementation should take 2,000 IU of vitamin D3 during pregnancy. Once born the first-degree relative of an MS patient will continue to require vitamin D3 supplementation based on weight. If the average amount required for an adult is 5,000 IU (50 kg) then a 5 kg infant requires one tenth this dose or 500 IU of vitamin D3 per day. Of course, sunlight is also a source of vitamin D3 during the summer months but there is some evidence that sunlight exposure is no longer achieving the desired 25(OH)D levels. Therefore, it is important to maintain vitamin D3 supplementation unless it is demonstrated that you are able to maintain levels greater than 40 ng/ml year round. The important point is to take enough Vitamin D3 supplement to maintain target levels greater than 40 ng/ml. To do this will require periodic blood tests to check 25(OH)D levels. 2. A recent meta analysis of 14 studies shows that being a smoker at any time increases the risk of MS by 50% compared to never smoking. This effect seems to be dose dependent (among and duration of smoking) and particularly strong in adolescence or early adulthood. Although smoking is on the decline there is a disturbing continued tendency for children, adolescents and young adults to experiment with smoking. It is extremely important for children and young adults who have first-degree relatives with MS to learn that any smoking must be avoided. This includes second hand smoke among other individuals in the household. The American Lung Association has an on line program called, “Freedom from Smoking” that is a good starting point for individuals interested in achieving this goal. It is also adapted to both adolescents and adults. 3. More recent evidence suggests that obesity is associated with the risk of developing MS. This risk is particularly strong if you inherit HLA haplotypes (genes) associated with MS. Therefore, diets and exercise programs to improve aerobic fitness and decrease excess weight are important not only for MS patients but essential for first-degree relatives of MS patients. Let us hope that by instituting these preventative measures we are able to not only decrease the risk of developing MS among your at risk relatives but also decrease the severity of the MS that may still develop in these family members. The next step will be the development of vaccines to control Epstein Barr Virus or mitigate the long-term effects of EBV infection. -Ben Greenberg, MD, MHS and Rip Kinkel, MD Benjamin M. Greenberg, MD, MHS Director, Transverse Myelitis, Neuromyelitis Optica and Pediatric Demyelinating Disease Programs Director, Neurosciences Clinical Research Center Department of Neurology and Neurotherapeutics Department of Pediatrics UT Southwestern  “The main facts in human life are five: birth, food, sleep, love and death.” ― E.M. Forster “I wonder why I don't go to bed and go to sleep. But then it would be tomorrow, so I decide that no matter how tired, no matter how incoherent I am, I can skip on hour more of sleep and live.” ― Sylvia Plath, The Unabridged Journals of Sylvia Plath Why do we so often forget how to sleep, as we grow older? Even without a chronic disease like Multiple Sclerosis our lifestyles and the changes to our body with aging conspire to interfere with restful sleep. Ask any woman going through menopause about their sleep and you will hear frustrating tales of awakenings for a variety of reasons many unexplained. Even well before the onslaught of middle age, our lifestyles become a hazard to sleep; we find ourselves with too little time between work and family responsibilities to take proper care of themselves. We stop exercising regularly, eat poorly, worry excessively and consume various drugs, some prescribed and others like alcohol and nicotine used to melt away our stresses and the burdens of feeling overwhelmed. Bad habits are formed early and persist. As the quote by Sylvia Plath (by the way she is not a good person from whom you should take advice regarding sleep) implies, from a young age we learn to burn the midnight candle too often and attempt to emulate those who never seem to require sleep. As people grow older they often develop strange beliefs or habits that actually worsen their sleep; some come to believe that they cannot fall asleep without the TV on or without a sleep aid and never attempt to adjust their sleep behavior. Often the problem is simply a result of a chronically disrupted circadian rhythm, yet the person insists it is simply impossible for them to fall asleep before 2 or 3 am. For people with MS, the problems with sleep are all too often blamed on the disease and simple measures are not attempted to control the insomnia before resorting to sleep aides or treatment of MS related symptoms perceived to be interfering with sleep. The cure for insomnia in MS patients and the excessive daytime sleepiness that it creates begins with the doctor taking a good history and patient being receptive to changing their current sleep behaviors. First, without excessive daytime sleepiness there is rarely a problem that requires treatment. Some people just require less sleep as they grow older; fewer still never require much sleep, yet never experience problems with feeling excessive sleepy during the day. With this caveat in mind it is often useful to separate sleep problems into three categories: those associated with sleep onset insomnia, those associated with nocturnal awakenings and those without perceived insomnia or awakenings but clearly creating excessive daytime sleepiness. Sleep onset insomnia (failure to get to sleep initially) is most often due to acute stressors, anxiety, depression (unipolar or bipolar), drugs (e.g. alcohol, stimulants including nicotine), eating large meals too late, pain, spasms when lying supine, restless legs syndrome or a disrupted circadian rhythm. These problems tend to be easy to identify and solve although they often require a willingness to change sleep behaviors (see list below). Medication to help with sleep onset insomnia is sometimes needed but only for short-term use. Long term use of medications to help with sleep should only be used after a complete evaluation. The same problems associated with sleep onset insomnia may also be responsible for awakenings during sleep, although the list becomes even longer with the inclusion of nocturnal awakenings to urinate because of bladder dysfunction, the co-existence of other medical conditions that interfere with sleep (Diabetes, lung disease, congestive heart failure etc.) and nocturnal hypoventilation in more severely disabled MS patients. The third category, excessive daytime sleepiness without perceived awakening, is often the result of a primary or secondary sleep disorder (obstructive sleep apnea, narcolepsy, nocturnal myoclonus, periodic limb movements of sleep) although your sleep partner is often able to provide the key history of snoring, suddenly disrupted breathing or leg movements that interfere with their sleep! Nocturnal hypoventilation can also present with feeling un-refreshed, confused and anxious on awakening because of not getting enough oxygen during sleep. As you have probably guessed by now, there is rarely one cause for your interrupted sleep and excessive daytime sleepiness. MS itself is often associated with daytime fatigue, a similar concept, but patients rarely describe this “fatigue” as the kind of daytime sleepiness one experiences after a bad night of sleep. Instead, MS fatigue is usually described as malaise, lassitude or an inability to move or think further without rest, more often without the craving to sleep during the day. The difficulty in diagnosis arises when a person experiences both daytime primary MS related fatigue and excessive sleepiness from disrupted sleep. So how should you manage your disrupted sleep? First, determine if your circadian rhythm is disrupted. This is usually obvious if you chronically find yourself unable to sleep until the middle of the night and then feel exhausted during the day because of the need to get up sooner than you would like. You will need to follow the advice listed below to improve your sleep hygiene but you may also need help in resetting your body’s clock; some people find success in resetting their clock by taking 3 mg of melatonin (an over the counter medication available at almost any pharmacy or supplement store) 2 hours before you would like to go to sleep. If this does not work after a week discuss the problem further with your physician. Rarely, a sleep specialist is needed to help people with chronic idiopathic (meaning unknown cause) insomnia. Next, you will need to adhere to the following steps to improve your sleep hygiene. This can be surprisingly difficult since many of us break these rules with regularity.
Lastly, if your problem with sleep or excessive daytime sleepiness is not easily managed with these adjustments or you are unable to follow through with these suggestions because of your MS or other medical problems, you will need to discuss these problems further with your primary care doctor or MS specialist. Common additional solutions may require treatment of depression, treatments of bladder problems to limit nocturnal awakening to urinate and treatment of pain and nocturnal spasms. A good sleep history should be obtained; it is often advisable to obtain a polysomnogram (also called a sleep study) and possibly an MSLT (multiple sleep latency test) if there is any suggestion of a sleep disorder or if attempts at treatment the insomnia fail to cure your excessive daytime sleepiness. “Suenos con los angeles” -Rip Kinkel, MD  Okay I will admit that the author is a good friend, but I highly recommend that anyone interested in learning more about the food they eat become acquainted with Louisa Kasdon’s Lets Talk About Food movement. Louisa, an accomplished writer, journalist and former food critic regularly posts information and recipes that are engaging, amusing and informative. While many of the posts will be most pertinent to those who reside in the Boston area, I have continued to follow and learn from her postings since moving to San Diego (https://www.facebook.com/LTAFood). I only wish I could attend the screening of Fed Up, the documentary by Katie Couric and Laurie David (An Inconvenient Truth) at Kendall Square Cinema later on April 24th. If you do miss the screening it will be opening in theater’s on May 9th. The more you become informed, the more you will realize how important diet is to your current and future health. You will also learn that it can be fun, if not easy, to change old habits. Hat’s off to a job well done. As is the case with politics, this may be why we need more women in the food industry -- Rip Kinkel, MD  We have talked about devices that assist people with foot drop, but what do you do when your leg becomes so weak in the hip flexor or knee flexor muscles that you can not lift the leg well enough to bring it forward while walking or going up and down steps? Or if you fatigue so rapidly that you can not walk for more than a short distance? One possible solution is the Hip Flexion Assist Device (HFAD) shown in this picture. Essentially this is a strong weight lifting belt with two attached elastic bungee cords that attach to your shoe. Make sure you order the type with a horizontal connecting strap that goes behind the knee. The mechanical principle of the device is simple; extending the leg at the hip loads the bungee cord so that when you attempt to bring the leg forward, the cord contracts and helps lift the leg at the hip. Now it may not be the most attractive contraption but it does work and is relatively cost effective. You will need a prescription from your doctor and some training on the use of the device by your physical therapist. If you are interested in learning more, go to the following site for information: http://www.beckerortho.com/AffiliatedCompanies/BTMRehab/Btmhfad.html |
DISCLAIMER:
The medical information and opinions on this site are provided as an information resource only, and are not to be used or relied on for any diagnostic or treatment purposes. The information and opinions expressed do not create any patient-physician relationship, and should not be used as a substitute for professional diagnosis and treatment. Please consult your health care provider before making any healthcare decisions or for guidance about a specific medical condition. Archives
January 2020
Categories
All
|
- Home
- About Us
- Virtual MS Center
- News & Resources
- Seminar Registration
- Health & Wellness
- Blogs
- About MS
-
Symptoms
- Balance and Walking Issues
- Breathing/Respiratory
- Bowel Dysfunction
- Cognitive Dysfunction
- Crying/Laughing Uncontrollably (PBA)
- Depression and Anxiety
- Dizziness/Vertigo
- Dysphagia
- Fatigue
- Foot Drop
- Hearing or Smell or Taste Changes
- Heat Sensitivity
- Leg Weakness
- Loss of Hand Dexterity and Coordination
- Memory and Mutliple Sclerosis
- Migraines
- Numbness/Tingling/Altered Sensation
- Nystagmus and Oscillopsia
- Pain
- Sexual Dysfunction
- Sleep Issues
- Spasticity/Spasms/Cramps
- Speech/Swallowing
- Urination/Bowel Problems
- Vision
- MS Clinics
- MS Topics
- Register With Us
- Terms of Use/Privacy/HIPAA
- MS HealthCare Journey
 RSS Feed
RSS Feed