|
I’ve always enjoyed the “Idiots Guide” series of books and wouldn’t be surprised if there were already one available on bladder function. My intention today is to provide a brief introduction of how your bladder is supposed to work and what often goes wrong in MS. 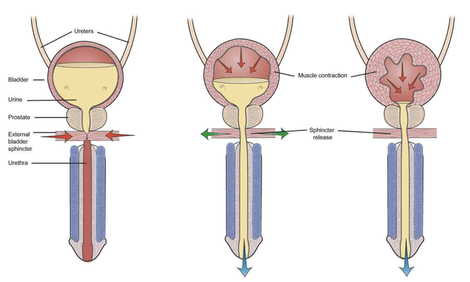 I stole the above diagram off the Internet for purposes of discussion. For woman in the audience, just remove the prostate and the penis and everything else is about the same.
1. Normal bladder function: The bladder is a hollow muscle (called the detrusor muscle) under autonomic nervous system control. This means that it is not directly under your conscious control like the muscles in your legs or arms. Urine flows from the kidneys (not shown) and down the ureters, which are the tubes connecting the kidney and the bladder. Normally, as the bladder fills with urine (left sided picture), the autonomic nervous system (parasympathetic type for those interested in details) prevents the bladder muscle (called the detrusor muscle) from contracting to squeeze out the urine and maintains a lower pressure in the bladder compared to the urethra. The urethra, by the way, is the tube through which urine flows out of you, preferably into the toilet. The pressure in this urethra is kept high by constant contraction of the external urinary sphincter and pelvic floor muscles. This prevents your urine from leaking or emptying spontaneously [note that there is also an internal urinary sphincter not shown in this picture that is also involved in urinary control but we can skip this for the basic discussion. In the diagram above the internal sphincter is located above the prostate in the bladder neck]. When you develop the urge to urinate, there is simultaneous contraction of the bladder detrusor muscle and relaxation the external urinary sphincter allowing urine to flow out smoothly. This coordinated activity is organized in a part of your brain called the pons (part of the brainstem). 2. Failure to store urine (detrusor over activity): This is probably the most common type of problem in people with MS. When MS involves the spinal cord, the detrusor muscle may become overactive. This is because of nerve fibers in the wall of the bladder that sense the stretching of the bladder as it fills, which stimulate neurons in the lower part of the spinal cord through a reflex to cause the bladder muscle to contract. You notice this as symptoms of early filling, urgency, frequency and incontinence when severe. The typical treatment is the use of a class of drugs called anti-muscarinic agents. These drugs work on the parasympathetic nervous system and prevent reflex contraction of the bladder. Common drugs used for this purpose include tolteridone (Detrol), oxybutynin (Ditropan), solifenicin (Vesicare), trospium (Sanctura), darifenacin (Enablex), fesoterodine (Toviaz). There are pros and cons to each of these drugs but all can cause a dry mouth, constipation and less commonly visual blurring. A new drug called Mirabegron (Myrbetriq), is a beta-3 adrenergic agonist that directly inhibits the signals being sent from the bladder to the spinal cord and allows the bladder to fill without contracting. Because it has a different mechanism of action from the anti-muscarinic drugs, we can use it in combination with these drugs in difficult to treat patients. 3. Failure to store and failure to empty (detrusor sphincter dysynergia or DSD): This is probably the second most common problem in MS patients. Imagine your bladder is a balloon filled with air and the opening in the balloon is your urinary sphincter. DSD occurs when there is no coordinated opening of the balloon to let out the air as you squeeze on the balloon with your other hand. In the case of your bladder you experience symptoms such as hesitancy and a poor urinary stream. You may also experience a feeling of not emptying completely (you are correct by the way) and a need to double void, meaning you think you are done but as soon as you get off the toilet or start to leave the bathroom you realize you still need to urinate more. Now your bladder does not have the same elastic properties of a balloon and people with DSD often leave a significant amount of urine in the bladder after they pee because the pressure in the bladder drops below the pressure in the urethra before you empty the bladder. This problem (failure to empty urine) is combined with the problem described previously (failure to store urine) to create urinary frequency, urgency, hesitancy, retention and the need to get up multiple times at night to pee. You may also experience various amounts of incontinence, depending on the severity of your problem, and frequent urinary tract infections because of the failure to flush urine out of the bladder (urine is a great culture medium for bacteria). Treatment involves managing the detrusor over activity with the drugs mentioned above (the anti-muscarinic agents) and trying to relax the urinary sphincter with a different set of medications that often don’t work very well. The medications for the dyregulated urinary sphincter (DSD) include drugs like tamsulosin (Flomax), doxazocin (Cardura) and terazocin (Hytrin). They should sound familiar to most middle-aged men since they are primarily use for prostatic enlargement, which causes similar symptoms. Anti-spasticity medications like baclofen and tizanidine are also sometimes used to treat DSD with variable success. Unfortunately, medications often do not work well for DSD and many people with MS continue to retain urine and experience incontinence and disrupted daily activities from frequent trips to the bathroom. If the amount of urine retained in the bladder is consistently over 100 cc, many physicians will advise intermittent self-catheterization. I usually recommend this only in patients with significantly disrupted lives, frequent incontinence or frequent urinary tract infections. For those with continued problems despite the strategies listed above, there are a number of newer therapeutic approaches that work well including intra-vesicular injection (meaning injection into the internal bladder wall through a procedure called cystoscopy) of Botox, a procedure done quickly in the urologists outpatient office every 3-6 months, neuromodulation with the InterStim® device and various surgical procedures that can often be performed with minimally invasive techniques. These procedures do require specialty management with a urologist. 4. Failure to Empty Urine: This is actually a rare isolated problem in MS and only seen with severe destruction of the lower spinal cord and sacral nerve roots. More often this occurs temporarily because of medication side effect or after a surgical procedure. This problem can only be solved with intermittent self-catheterization since the bladder wall is not able to contract and empty urine. So there you have it; the basics of bladder function and the problems that occur in MS. In future posts we will discuss practical issues such as the pros and cons of different type of catheters, how to avoid chronic Foley catheters, and how to stay dry. Stay tuned... Dr. Kinkel 7/1/2014 10:36:41 pm
Thanks for providing very effective information that will surely help the MS Patients.
Lizzz
4/22/2016 08:47:45 pm
Thank you. First appt with urologist today- this was a great blog to find. Dix with ms in '10. Comments are closed.
|
DISCLAIMER:
The medical information and opinions on this site are provided as an information resource only, and are not to be used or relied on for any diagnostic or treatment purposes. The information and opinions expressed do not create any patient-physician relationship, and should not be used as a substitute for professional diagnosis and treatment. Please consult your health care provider before making any healthcare decisions or for guidance about a specific medical condition. Archives
January 2020
Categories
All
|
- Home
- About Us
- Virtual MS Center
- News & Resources
- Seminar Registration
- Health & Wellness
- Blogs
- About MS
-
Symptoms
- Balance and Walking Issues
- Breathing/Respiratory
- Bowel Dysfunction
- Cognitive Dysfunction
- Crying/Laughing Uncontrollably (PBA)
- Depression and Anxiety
- Dizziness/Vertigo
- Dysphagia
- Fatigue
- Foot Drop
- Hearing or Smell or Taste Changes
- Heat Sensitivity
- Leg Weakness
- Loss of Hand Dexterity and Coordination
- Memory and Mutliple Sclerosis
- Migraines
- Numbness/Tingling/Altered Sensation
- Nystagmus and Oscillopsia
- Pain
- Sexual Dysfunction
- Sleep Issues
- Spasticity/Spasms/Cramps
- Speech/Swallowing
- Urination/Bowel Problems
- Vision
- MS Clinics
- MS Topics
- Register With Us
- Terms of Use/Privacy/HIPAA
- MS HealthCare Journey
 RSS Feed
RSS Feed